
Volume 20, Issue 2 (10-2023)
J Res Dev Nurs Midw 2023, 20(2): 26-29 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Haji Hoseini N, Borghei N S, Reyhani M, Tatari M. A study on the effect of husbands' attendance in the delivery ward on the duration of labor and mode of delivery in primigravid women. J Res Dev Nurs Midw 2023; 20 (2) :26-29
URL: http://nmj.goums.ac.ir/article-1-1442-en.html
URL: http://nmj.goums.ac.ir/article-1-1442-en.html



1- Counseling and Reproductive Health Research Center, School of Nursing and Midwifery, Golestan University of Medical Sciences, Gorgan, Iran
2- Counseling and Reproductive Health Research Center, School of Nursing and Midwifery, Golestan University of Medical Sciences, Gorgan, Iran ,borghei2006@yahoo.com
2- Counseling and Reproductive Health Research Center, School of Nursing and Midwifery, Golestan University of Medical Sciences, Gorgan, Iran ,
Full-Text [PDF 447 kb]
(1165 Downloads)
| Abstract (HTML) (2129 Views)
.png)
Discussion
The present study aimed to explore the impact of husbands' presence in the delivery ward on the duration of the active phase of labor among patients at Kalaleh Hospital's maternity center. According to the findings, no correlation was observed between the husbands' presence in the delivery ward and the duration of the active phase of labor. Furthermore, this presence did not influence the delivery method or any labor interventions. Gungor et al. found no relationship between paternal support and the duration of labor or midwifery interventions during childbirth in a study examining the effect of husbands' presence in the delivery ward on their wives' childbirth experiences (14). Similarly, Carter's research indicated that husbands' presence did not affect the duration of labor (13), a result that aligns with the findings of this study.
Due to the limited number of studies evaluating the effect of husbands' presence in the delivery ward on the duration of labor, the results of the present study were compared with those focusing on the general impact of attendance in the delivery ward. For instance, Nobakht et al. assessed the effect of a companion's presence on labor duration in primigravid women. They concluded no significant difference between the experimental and control groups regarding the duration of the active phase of labor (20). Various other studies have examined the influence of a supportive attendant during labor and found such presence inconsequential. Dadshahi et al. reported that the presence of a midwife did not yield a statistically significant difference between the experimental and control groups concerning the use of oxytocin or the type of delivery (21). Bruggemann found that women supported by a midwife during labor did not exhibit a statistically significant difference in labor duration compared to those without support (22), consistent with the present study.
However, some research has highlighted the positive effects of a companion's presence in the delivery ward on labor progression. For example, Khanvandizadeh et al. noted that a midwife's presence from admission until delivery reduced the duration of labor (16). Darvishi et al. also discovered that a midwife's attendance, as opposed to a non- midwife's, led to a more substantial reduction in labor duration and lessened the need for oxytocin (15). Given that these studies evaluated the impact of a trained midwife (or doula), the presence of an experienced individual has a more significant effect on labor progress than that of the husband. In this study, although the duration of the active phase of labor was lower among women whose husbands were present in the delivery ward compared to those without, the difference was not statistically significant. Therefore, future research is recommended to examine the impact of husbands who are adequately trained to support their wives during labor-on-labor progression in Iran. Thomas's study suggested that husbands could offer emotional and informed support to their wives if adequately educated about pregnancy and childbirth (8). Salehi et al. also emphasized the importance of a trained husband's presence during childbirth (23). Educating husbands, particularly first-time fathers, could enable them to play an active and meaningful role during delivery and childbirth (24).
In examining the impact of an attendant's presence on the delivery method, Rostampey et al. found that attendance did not influence the choice of delivery method, as all the women in their study had vaginal deliveries (19). Similarly, our current study revealed that most participants in both groups also had vaginal deliveries. No significant differences were noted between the two groups regarding delivery method. This lack of variation could be attributed to the study's inclusion criteria, which mandated that participants be in the active phase of labor. Consequently, the likelihood of vaginal delivery increases when mothers are given sufficient time to progress to this active phase. Encouraging expectant mothers, particularly those experiencing their first pregnancy, to reach the active labor phase could effectively increase the rate of vaginal deliveries.
Another aspect worth considering is the couple's willingness to have the husband present in the delivery ward. Adeyemi et al.'s study in Nigeria indicated that many couples held negative views about the husband's presence during delivery, primarily due to inadequate training in this area (25). Moreover, a husband's presence can sometimes induce stress and anxiety for the woman. Given the potential significance of a husband's involvement in childbirth, it is essential to establish programs that prepare men for active participation. These programs should explain why and how they should be involved, what roles they can assume, and the extent of their participation, all while considering various social and cultural factors (26). Johnson et al.'s meta-analysis found that most husbands felt committed to and vulnerable during childbirth. They emphasized that adequate preparation and support are crucial for husbands, who should be allowed to define their roles during labor and delivery. However, if a husband prefers not to attend, his decision should be respected (27). In line with these findings, consent forms were signed by all participating couples in both groups regarding the husband's presence in the delivery ward. Thus, securing the wife's consent for her husband's attendance—provided he is willing to be there—can contribute to a more pleasant childbirth experience.
A further challenge is institutional resistance to allowing husbands in the delivery ward. Despite the acknowledged benefits of a spouse's or companion's presence during labor, most maternity hospitals still prohibit it due to legal and health concerns, thereby overlooking its importance. Encouraging midwives and healthcare providers to engage husbands during prenatal care could prepare new fathers for active participation in childbirth and address the challenges surrounding their presence in delivery wards. Wu et al. identified several barriers to a husband's presence, including the level of information and attitude toward participation, the quality of the marital relationship, and various demographic factors such as age, education level, job status, number of children, and place of residence (28). Additional constraints, such as health guidelines stemming from the COVID-19 pandemic, crowded delivery wards, work-related issues, and scheduling conflicts between the husband's work hours and the wife's hospitalization, also play a role. Therefore, overcoming these barriers is essential to allow all couples a fulfilling childbirth experience, should they desire their husbands' presence.
Conclusion
The research findings suggest that a husband's presence in the delivery ward does not influence the duration or method of childbirth. Despite the numerous advantages associated with vaginal delivery and the relatively low rate of husbands attending delivery wards, further research is needed to explore the impacts of their presence. Accordingly, future studies should examine other dimensions of a husband's attendance, such as its effects on marital satisfaction, sexual satisfaction, postpartum stress and depression, involvement in newborn care, and breastfeeding success.
Acknowledgement
This article originated from a master's thesis in midwifery counseling of the Nursing & Midwifery Faculty. The authors thank the Research and Technology Deputy of Golestan University of Medical Sciences for approving and financially supporting this research project. We also extend our thanks to all participants who contributed to the successful completion of this study.
Funding sources
The Vice-Chancellor for Research and Technology, Golestan University of Medical Sciences, has funded the original research.
Ethical statement
The research project received approval from the Research System of Golestan University of Medical Sciences, under approval number 111562-16, and the regional ethics committee, with the ethical code IR.GOUMS.REC.1399.231. It was also registered in the Iranian Registry of Clinical Trials (IRCT) under registration number 20180408039229N2.
Conflicts of interest
The authors declare that there is no conflict of interest.
Author contributions
Borghei Narjes Sadat: made substantial contributions to the conception / design of the work; Mitra Reyhani: made substantial contributions to the conception; Nahid Haji Hoseini: interpretation of data, have drafted the work or substantively revised it and Mahin Tatari: the acquisition, analysis.
Full-Text: (430 Views)
Introduction
Women encounter various anxiety-inducing events throughout their lives, among which pregnancy and childbirth are particularly significant (1). To mitigate these anxieties, governments initiate numerous programs, one of which involves the active participation of family members during childbirth (2). According to health organizations, achieving the Millennium Development Goals (MDGs) necessitates focusing on reproductive health, a sphere in which the husband's involvement is instrumental (3). Such participation is especially vital for reducing maternal mortality in societies where men are the primary decision-makers within the family (4).
The husband is often the most responsible family member during pregnancy and childbirth, playing a critical role in supporting his wife throughout this period (2). His involvement can substantially alleviate anxiety in expectant mothers (1). Some studies even suggest that emotional support from the husband can significantly reduce pain and stress during childbirth, enhancing pregnancy outcomes (5).
In Iran, however, it is relatively uncommon for husbands to be involved in matters related to pregnancy and childbirth (6). Despite a growing desire among men to be well-informed about the challenges women face during pregnancy and to accompany their wives during prenatal care, numerous obstacles prevent their active participation (7). Over the years, more men have been willing to learn about women's health issues during pregnancy and to accompany their wives during medical appointments (8). The active involvement of husbands not only enhances the quality of marital relationships but also has a positive impact on reducing both maternal and infant mortality rates (9). Consequently, most women prefer their husbands' companionship throughout pregnancy and childbirth care, particularly during initial visits (10, 11).
While most women and a significant portion of men advocate for the husband's presence in the delivery ward (12), existing research yields conflicting results regarding its impact on childbirth. Some studies have found no correlation between the husband's presence and the duration of labor nor the use of analgesics and surgical interventions (13, 14). Systematic reviews and meta-analyses conducted in developing countries have yet to offer conclusive evidence supporting the benefits of a husband's presence in the delivery ward (5). Furthermore, although some studies confirm the positive influence of a non-husband attendant on labor duration (15, 16), research conducted in Saudi Arabia indicates that a husband's attendance, while not widespread, is crucial for providing emotional support and fostering an optimal marital relationship (17).
In light of the potential benefits of husbands' involvement in childbirth-aligned with national health objectives such as the youth population program, promotion of vaginal delivery, and childbearing-it becomes essential to explore this topic further. Given the absence of studies focusing on the effects of husbands' attendance in the delivery wards within the cultural context of the easternmost county of Golestan Province, this study aims to examine the impact of such attendance on the duration of labor in primigravid women.
Methods
The current study was an interventional field trial that assessed 57 couples who visited Rasoul Akram Hospital for their first pregnancies in 2021. Participants were divided into intervention (28 couples) and control (29 couples) groups using a randomized block design with quad-number blocks.
The inclusion criteria consisted of Iranian citizenship, proficiency in reading, speaking, writing, and understanding Persian, confirmed fetal health based on available records, and eligibility for vaginal delivery-such as hospital admission at the onset of the active labor phase (cervical dilation of 3-5 cm)—a gestational age between 38 and 42 weeks, the presence of a singleton and live fetus, a planned pregnancy, willingness for the husband to be present in the delivery ward, and mutual marital consent. Exclusion criteria included a husband's refusal to remain in the delivery ward for at least two hours and early cesarean section (occurring less than two hours after hospital admission).
Sampling targeted husbands of primigravid women who visited the maternity center at Rasoul Akram Hospital in Kalaleh County, Golestan Province, Iran. Men who consented to participate in the study, to be present in the delivery ward, and whose wives met the inclusion criteria were enrolled. They were briefed for 15 minutes in the hospital's conference hall on the study objectives and health and care principles to follow during labor. Before study enrollment, husbands were required to obtain their wives' consent for their presence, verified through written informed consent forms. As for research randomization, participants were informed that they had an equal chance of being placed in either the intervention or control group, with only the former allowed to attend the delivery ward with their wives.
Regarding sample allocation, participants were assigned to one of several block permutations (AABB-ABAB-ABBA-BABA-BAAB-BBAA), where 'A' represented the intervention group and 'B' was the control group. Blocks were chosen using a simple randomized method without permutation. Participants were allocated to their respective groups according to the selected block's permutations, continuing until the sample size for each group was reached.
The content validity of the labor progress checklist-which included cervical dilation, effacement, fetal heart rate records in the patient file, and the partograph curve—was affirmed through consultation with 10 midwifery professors at the Faculty of Nursing and Midwifery. Entry into the active labor phase was defined by a minimum cervical dilation of 3 cm and an active dilation rate of at least 1.2 cm per hour. The researcher carried out all sampling procedures while the maternity center's midwives completed the labor progress sheet in the researcher's presence. Given the separate labor, delivery, and recovery (LDR) rooms for the intervention and control groups and the absence of interaction, there was no need for a placebo. The control group received standard ward care, whereas the intervention group benefited from the husband's presence in the delivery ward for at least two hours.
Due to the COVID-19 pandemic, all pregnancy-related classes were suspended, and none of the study participants could attend these sessions. The research instruments used included a demographic and delivery characteristics questionnaire, a labor progress questionnaire, and the ENRICH couple scale.
The ENRICH couple scale was initially developed by Fowers and Olson in 1989 to assess levels of marital satisfaction. Asoudeh et al. (2010) later validated and approved a 35-item version of this tool for its reliability and validity. The scale employs a 5-point Likert system, ranging from 1 (strongly disagree) to 5 (strongly agree). It comprehensively measures various aspects of marital relationships, including satisfaction, communication, ideal distortion, and conflict resolution. In Asoudeh's study, the scale demonstrated an alpha value of 0.78. The reliability coefficient was determined to be 0.84 (18) using the split-half method.
Based on research by Rostampey et al. (19) and utilizing the sample size equation with a confidence level of 0.95 and a statistical power of 80%, the required sample size was calculated to be 27 individuals per group. To account for a 10% attrition rate for each group, we set the total sample size at 60 participants.
Of the 60 participants, two individuals from the intervention group were excluded due to their presence in the delivery ward for less than two hours. Additionally, one individual from the control group was removed because of an unwillingness to continue participation. Consequently, statistical analyses were conducted on the remaining 57 participants: 28 in the intervention group and 29 in the control group (Figure 1).
Women encounter various anxiety-inducing events throughout their lives, among which pregnancy and childbirth are particularly significant (1). To mitigate these anxieties, governments initiate numerous programs, one of which involves the active participation of family members during childbirth (2). According to health organizations, achieving the Millennium Development Goals (MDGs) necessitates focusing on reproductive health, a sphere in which the husband's involvement is instrumental (3). Such participation is especially vital for reducing maternal mortality in societies where men are the primary decision-makers within the family (4).
The husband is often the most responsible family member during pregnancy and childbirth, playing a critical role in supporting his wife throughout this period (2). His involvement can substantially alleviate anxiety in expectant mothers (1). Some studies even suggest that emotional support from the husband can significantly reduce pain and stress during childbirth, enhancing pregnancy outcomes (5).
In Iran, however, it is relatively uncommon for husbands to be involved in matters related to pregnancy and childbirth (6). Despite a growing desire among men to be well-informed about the challenges women face during pregnancy and to accompany their wives during prenatal care, numerous obstacles prevent their active participation (7). Over the years, more men have been willing to learn about women's health issues during pregnancy and to accompany their wives during medical appointments (8). The active involvement of husbands not only enhances the quality of marital relationships but also has a positive impact on reducing both maternal and infant mortality rates (9). Consequently, most women prefer their husbands' companionship throughout pregnancy and childbirth care, particularly during initial visits (10, 11).
While most women and a significant portion of men advocate for the husband's presence in the delivery ward (12), existing research yields conflicting results regarding its impact on childbirth. Some studies have found no correlation between the husband's presence and the duration of labor nor the use of analgesics and surgical interventions (13, 14). Systematic reviews and meta-analyses conducted in developing countries have yet to offer conclusive evidence supporting the benefits of a husband's presence in the delivery ward (5). Furthermore, although some studies confirm the positive influence of a non-husband attendant on labor duration (15, 16), research conducted in Saudi Arabia indicates that a husband's attendance, while not widespread, is crucial for providing emotional support and fostering an optimal marital relationship (17).
In light of the potential benefits of husbands' involvement in childbirth-aligned with national health objectives such as the youth population program, promotion of vaginal delivery, and childbearing-it becomes essential to explore this topic further. Given the absence of studies focusing on the effects of husbands' attendance in the delivery wards within the cultural context of the easternmost county of Golestan Province, this study aims to examine the impact of such attendance on the duration of labor in primigravid women.
Methods
The current study was an interventional field trial that assessed 57 couples who visited Rasoul Akram Hospital for their first pregnancies in 2021. Participants were divided into intervention (28 couples) and control (29 couples) groups using a randomized block design with quad-number blocks.
The inclusion criteria consisted of Iranian citizenship, proficiency in reading, speaking, writing, and understanding Persian, confirmed fetal health based on available records, and eligibility for vaginal delivery-such as hospital admission at the onset of the active labor phase (cervical dilation of 3-5 cm)—a gestational age between 38 and 42 weeks, the presence of a singleton and live fetus, a planned pregnancy, willingness for the husband to be present in the delivery ward, and mutual marital consent. Exclusion criteria included a husband's refusal to remain in the delivery ward for at least two hours and early cesarean section (occurring less than two hours after hospital admission).
Sampling targeted husbands of primigravid women who visited the maternity center at Rasoul Akram Hospital in Kalaleh County, Golestan Province, Iran. Men who consented to participate in the study, to be present in the delivery ward, and whose wives met the inclusion criteria were enrolled. They were briefed for 15 minutes in the hospital's conference hall on the study objectives and health and care principles to follow during labor. Before study enrollment, husbands were required to obtain their wives' consent for their presence, verified through written informed consent forms. As for research randomization, participants were informed that they had an equal chance of being placed in either the intervention or control group, with only the former allowed to attend the delivery ward with their wives.
Regarding sample allocation, participants were assigned to one of several block permutations (AABB-ABAB-ABBA-BABA-BAAB-BBAA), where 'A' represented the intervention group and 'B' was the control group. Blocks were chosen using a simple randomized method without permutation. Participants were allocated to their respective groups according to the selected block's permutations, continuing until the sample size for each group was reached.
The content validity of the labor progress checklist-which included cervical dilation, effacement, fetal heart rate records in the patient file, and the partograph curve—was affirmed through consultation with 10 midwifery professors at the Faculty of Nursing and Midwifery. Entry into the active labor phase was defined by a minimum cervical dilation of 3 cm and an active dilation rate of at least 1.2 cm per hour. The researcher carried out all sampling procedures while the maternity center's midwives completed the labor progress sheet in the researcher's presence. Given the separate labor, delivery, and recovery (LDR) rooms for the intervention and control groups and the absence of interaction, there was no need for a placebo. The control group received standard ward care, whereas the intervention group benefited from the husband's presence in the delivery ward for at least two hours.
Due to the COVID-19 pandemic, all pregnancy-related classes were suspended, and none of the study participants could attend these sessions. The research instruments used included a demographic and delivery characteristics questionnaire, a labor progress questionnaire, and the ENRICH couple scale.
The ENRICH couple scale was initially developed by Fowers and Olson in 1989 to assess levels of marital satisfaction. Asoudeh et al. (2010) later validated and approved a 35-item version of this tool for its reliability and validity. The scale employs a 5-point Likert system, ranging from 1 (strongly disagree) to 5 (strongly agree). It comprehensively measures various aspects of marital relationships, including satisfaction, communication, ideal distortion, and conflict resolution. In Asoudeh's study, the scale demonstrated an alpha value of 0.78. The reliability coefficient was determined to be 0.84 (18) using the split-half method.
Based on research by Rostampey et al. (19) and utilizing the sample size equation with a confidence level of 0.95 and a statistical power of 80%, the required sample size was calculated to be 27 individuals per group. To account for a 10% attrition rate for each group, we set the total sample size at 60 participants.
Of the 60 participants, two individuals from the intervention group were excluded due to their presence in the delivery ward for less than two hours. Additionally, one individual from the control group was removed because of an unwillingness to continue participation. Consequently, statistical analyses were conducted on the remaining 57 participants: 28 in the intervention group and 29 in the control group (Figure 1).
For statistical analysis, SPSS 18 software was employed. The normality of the quantitative response variable was first assessed using the Shapiro-Wilk test, which confirmed its non-normal distribution. The Mann–Whitney U test was then used to compare the means of the two groups. Qualitative variables were analyzed using the Chi-square test and Fisher's exact test, set at a significance level 0.05. All ethical considerations were observed throughout the research process, including obtaining informed consent from participants and ensuring data confidentiality.
Results
The present study analyzed data from 57 participating couples. None of the participants had a history of infertility, and 96.6% of the pregnancies were planned. No statistically significant differences were observed between the two groups concerning their history of abortion and their desire for pregnancy.
Most women were housewives, resided in rural areas, had limited financial resources, held secondary school diplomas, and married self-employed husbands. The two groups had no statistically significant differences in these demographic variables (Table 1).
Results
The present study analyzed data from 57 participating couples. None of the participants had a history of infertility, and 96.6% of the pregnancies were planned. No statistically significant differences were observed between the two groups concerning their history of abortion and their desire for pregnancy.
Most women were housewives, resided in rural areas, had limited financial resources, held secondary school diplomas, and married self-employed husbands. The two groups had no statistically significant differences in these demographic variables (Table 1).
Table 1: Comparison of qualitative demographic variables between the control and intervention groups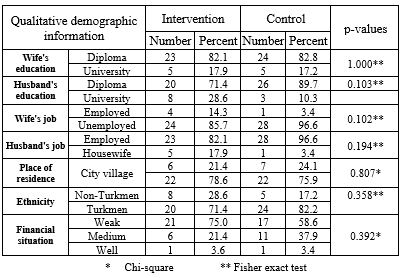 |
The average and standard deviation for marital satisfaction, age of the pregnant women, gestational age, and the duration of the active phase of labor showed no statistically significant differences between the intervention and control groups. The length of stay in the delivery ward was recorded solely in the intervention group, as it was a prerequisite for the intervention (Table 2).
Table 2: Comparison of mean quantitative variables between the control and intervention groups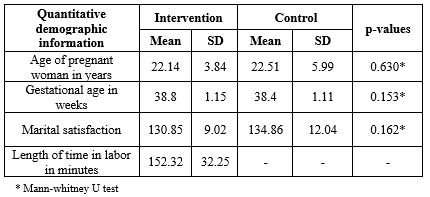 |
Analysis of the type of delivery and interventions during labor revealed that vaginal delivery was the most prevalent method in both groups. Moreover, 64.3% of the interventions during labor in the intervention group and 58.6% in the control group were of the induction type. No statistically significant differences concerning these variables were found between the two groups (Table 3).
Table 3: Frequency distribution of delivery type and interventions during labor in the control and intervention groups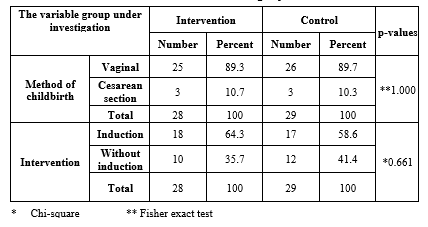 |
Finally, the average duration of the active phase of labor exhibited no statistically significant differences between the intervention and control groups (Table 4).
Table 4: Average durations of the active phase in the control and intervention groups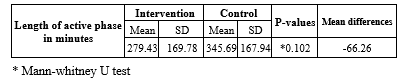 |
Discussion
The present study aimed to explore the impact of husbands' presence in the delivery ward on the duration of the active phase of labor among patients at Kalaleh Hospital's maternity center. According to the findings, no correlation was observed between the husbands' presence in the delivery ward and the duration of the active phase of labor. Furthermore, this presence did not influence the delivery method or any labor interventions. Gungor et al. found no relationship between paternal support and the duration of labor or midwifery interventions during childbirth in a study examining the effect of husbands' presence in the delivery ward on their wives' childbirth experiences (14). Similarly, Carter's research indicated that husbands' presence did not affect the duration of labor (13), a result that aligns with the findings of this study.
Due to the limited number of studies evaluating the effect of husbands' presence in the delivery ward on the duration of labor, the results of the present study were compared with those focusing on the general impact of attendance in the delivery ward. For instance, Nobakht et al. assessed the effect of a companion's presence on labor duration in primigravid women. They concluded no significant difference between the experimental and control groups regarding the duration of the active phase of labor (20). Various other studies have examined the influence of a supportive attendant during labor and found such presence inconsequential. Dadshahi et al. reported that the presence of a midwife did not yield a statistically significant difference between the experimental and control groups concerning the use of oxytocin or the type of delivery (21). Bruggemann found that women supported by a midwife during labor did not exhibit a statistically significant difference in labor duration compared to those without support (22), consistent with the present study.
However, some research has highlighted the positive effects of a companion's presence in the delivery ward on labor progression. For example, Khanvandizadeh et al. noted that a midwife's presence from admission until delivery reduced the duration of labor (16). Darvishi et al. also discovered that a midwife's attendance, as opposed to a non- midwife's, led to a more substantial reduction in labor duration and lessened the need for oxytocin (15). Given that these studies evaluated the impact of a trained midwife (or doula), the presence of an experienced individual has a more significant effect on labor progress than that of the husband. In this study, although the duration of the active phase of labor was lower among women whose husbands were present in the delivery ward compared to those without, the difference was not statistically significant. Therefore, future research is recommended to examine the impact of husbands who are adequately trained to support their wives during labor-on-labor progression in Iran. Thomas's study suggested that husbands could offer emotional and informed support to their wives if adequately educated about pregnancy and childbirth (8). Salehi et al. also emphasized the importance of a trained husband's presence during childbirth (23). Educating husbands, particularly first-time fathers, could enable them to play an active and meaningful role during delivery and childbirth (24).
In examining the impact of an attendant's presence on the delivery method, Rostampey et al. found that attendance did not influence the choice of delivery method, as all the women in their study had vaginal deliveries (19). Similarly, our current study revealed that most participants in both groups also had vaginal deliveries. No significant differences were noted between the two groups regarding delivery method. This lack of variation could be attributed to the study's inclusion criteria, which mandated that participants be in the active phase of labor. Consequently, the likelihood of vaginal delivery increases when mothers are given sufficient time to progress to this active phase. Encouraging expectant mothers, particularly those experiencing their first pregnancy, to reach the active labor phase could effectively increase the rate of vaginal deliveries.
Another aspect worth considering is the couple's willingness to have the husband present in the delivery ward. Adeyemi et al.'s study in Nigeria indicated that many couples held negative views about the husband's presence during delivery, primarily due to inadequate training in this area (25). Moreover, a husband's presence can sometimes induce stress and anxiety for the woman. Given the potential significance of a husband's involvement in childbirth, it is essential to establish programs that prepare men for active participation. These programs should explain why and how they should be involved, what roles they can assume, and the extent of their participation, all while considering various social and cultural factors (26). Johnson et al.'s meta-analysis found that most husbands felt committed to and vulnerable during childbirth. They emphasized that adequate preparation and support are crucial for husbands, who should be allowed to define their roles during labor and delivery. However, if a husband prefers not to attend, his decision should be respected (27). In line with these findings, consent forms were signed by all participating couples in both groups regarding the husband's presence in the delivery ward. Thus, securing the wife's consent for her husband's attendance—provided he is willing to be there—can contribute to a more pleasant childbirth experience.
A further challenge is institutional resistance to allowing husbands in the delivery ward. Despite the acknowledged benefits of a spouse's or companion's presence during labor, most maternity hospitals still prohibit it due to legal and health concerns, thereby overlooking its importance. Encouraging midwives and healthcare providers to engage husbands during prenatal care could prepare new fathers for active participation in childbirth and address the challenges surrounding their presence in delivery wards. Wu et al. identified several barriers to a husband's presence, including the level of information and attitude toward participation, the quality of the marital relationship, and various demographic factors such as age, education level, job status, number of children, and place of residence (28). Additional constraints, such as health guidelines stemming from the COVID-19 pandemic, crowded delivery wards, work-related issues, and scheduling conflicts between the husband's work hours and the wife's hospitalization, also play a role. Therefore, overcoming these barriers is essential to allow all couples a fulfilling childbirth experience, should they desire their husbands' presence.
Conclusion
The research findings suggest that a husband's presence in the delivery ward does not influence the duration or method of childbirth. Despite the numerous advantages associated with vaginal delivery and the relatively low rate of husbands attending delivery wards, further research is needed to explore the impacts of their presence. Accordingly, future studies should examine other dimensions of a husband's attendance, such as its effects on marital satisfaction, sexual satisfaction, postpartum stress and depression, involvement in newborn care, and breastfeeding success.
Acknowledgement
This article originated from a master's thesis in midwifery counseling of the Nursing & Midwifery Faculty. The authors thank the Research and Technology Deputy of Golestan University of Medical Sciences for approving and financially supporting this research project. We also extend our thanks to all participants who contributed to the successful completion of this study.
Funding sources
The Vice-Chancellor for Research and Technology, Golestan University of Medical Sciences, has funded the original research.
Ethical statement
The research project received approval from the Research System of Golestan University of Medical Sciences, under approval number 111562-16, and the regional ethics committee, with the ethical code IR.GOUMS.REC.1399.231. It was also registered in the Iranian Registry of Clinical Trials (IRCT) under registration number 20180408039229N2.
Conflicts of interest
The authors declare that there is no conflict of interest.
Author contributions
Borghei Narjes Sadat: made substantial contributions to the conception / design of the work; Mitra Reyhani: made substantial contributions to the conception; Nahid Haji Hoseini: interpretation of data, have drafted the work or substantively revised it and Mahin Tatari: the acquisition, analysis.
Type of study: Original Article |
Subject:
Midwifery
References
1. Syam A, Iskandar I, Qasim M, Kadir A, Usman AN. Identifying risk factors of prenatal depression among mothers in Indonesia. Enfermería clínica. 2020;30(S2):550-4. [View at Publisher] [DOI] [Google Scholar]
2. Rumaseuw R, Berliana SM, Nursalam N, Efendi F, Pradanie R, Rachmawati PD, et al., editors. Factors affecting husband participation in antenatal care attendance and delivery. IOP Conference Series: Earth and Environmental Science: IOP Publishing; 2018. [View at Publisher] [DOI] [Google Scholar]
3. Jamali F, Olfati F, Oveisi S, Ranjkesh F. Effects of spouses' involvement in pregnancy on fear of childbirth in nulliparous women. Journal of Inflammatory Diseases. 2018;22(2):38-47. [View at Publisher] [DOI] [Google Scholar]
4. Kashaija DK, Mselle LT, Mkoka DA. Husbands' experience and perception of supporting their wives during childbirth in Tanzania. BMC Pregnancy Childbirth. 2020;20(1):85. [View at Publisher] [DOI] [PMID] [Google Scholar]
5. Yargawa J, Leonardi-Bee J. Male involvement and maternal health outcomes: systematic review and meta-analysis. J Epidemiol Community Health. 2015;69(6):604-12. [View at Publisher] [DOI] [PMID] [Google Scholar]
6. Dehshiri M, Ghorashi Z, Lotfipur SM. Effects of Husband Involvement in Prenatal Care on Couples' Intimacy and Postpartum Blues in Primiparous Women: A Quasi-Experimental Study. Int J Community Based Nurs Midwifery. 2023;11(3):179-89. [View at Publisher] [DOI] [PMID] [Google Scholar]
7. Mehran N, Hajian S, Simbar M, Alavi Majd H. Spouse's participation in perinatal care: a qualitative study. BMC pregnancy childbirth. 2020;20(1):489. [View at Publisher] [DOI] [PMID] [Google Scholar]
8. Thomas GM, Lupton D, Pedersen S. 'The appy for a happy pappy': expectant fatherhood and pregnancy apps. Journal of Gender Studies. 2018;27(7):759-70. [View at Publisher] [DOI] [Google Scholar]
9. Arisukwu O, Igbolekwu CO, Oyekola IA, Oyeyipo EJ, Asamu FF, Osueke O. Spousal support during pregnancy in the Nigerian rural context: a mixed methods study. BMC Pregnancy Childbirth. 2021;21(1):772. [View at Publisher] [DOI] [PMID] [Google Scholar]
10. Maluka SO, Peneza AK. Perceptions on male involvement in pregnancy and childbirth in Masasi District, Tanzania: a qualitative study. Reprod Health. 2018;15(1):68. [View at Publisher] [DOI] [PMID] [Google Scholar]
11. Ndirima Z, Neuhann F, Beiersmann C. Listening to their voices: understanding rural women's perceptions of good delivery care at the Mibilizi District Hospital in Rwanda. BMC women's Health. 2018;18(1):38. [View at Publisher] [DOI] [PMID] [Google Scholar]
12. Fathnezhad Kazemi A, Sharifi N, Simbar M. A review on different aspects of men's participation in antenatal care. Jorjani Biomed J. 2017;5(1):1-13. [View at Publisher] [Google Scholar]
13. Carter MW, Speizer I. Salvadoran fathers' attendance at prenatal care, delivery, and postpartum care. Rev Panam Salud Publica. 2005;18(3):149-56. [View at Publisher] [DOI] [PMID] [Google Scholar]
14. Gungor I, Beji NK. Effects of fathers' attendance to labor and delivery on the experience of childbirth in Turkey. West J Nurs Res. 2007;29(2):213-31. [View at Publisher] [DOI] [PMID] [Google Scholar]
15. Darvishi M, Ranjbaran M, Jourabchi Z, Jafarimanesh H. Effect of the presence of midwife and non-midwife companion on labor pain, duration of delivery, and amount of oxytocin drops in primiparous women: a clinical trial study. The Iranian Journal of Obstetrics, Gynecology and Infertility. 2019;22(4):63-72. [View at Publisher] [DOI] [Google Scholar]
16. Khavandizadeh Aghdam S, Kazemzadeh R, Nikjoo R. The effect of the doula support during labor on delivery length in primigravida women. The Iranian Journal of Obstetrics, Gynecology and Infertility. 2015;18(150):8-13. [View at Publisher] [DOI] [PMID] [Google Scholar]
17. Alharbi AA, Alodhayani AA, Aldegether MS, Batais MA, Almigbal TH, Alyousefi NA. Attitudes and barriers toward the presence of husbands with their wives in the delivery room during childbirth in Riyadh, Saudi Arabia. J Family Med Prim Care. 2018;7(6):1467-75. [View at Publisher] [DOI] [PMID] [Google Scholar]
18. Rostampey Z, Khakbazan Z, Golestan B. Effect of Trained Female Relative on Active Phase Length during Labor among Low Risk Pregnancies. J Guilan Univ Med Sci. 2010;19(75):79-85. [View at Publisher] [Google Scholar]
19. Asoodeh MH, Khalili S, Daneshpour M, Lavasani MG. Factors of successful marriage: Accounts from self described happy couples. Procedia-Social and Behavioral Sciences. 2010;5:2042-6. [View at Publisher] [DOI] [Google Scholar]
20. Rafiee vL, Nobakht F, Safdari df, Parvin N. The effect of the presence of an attendant on anxiety and labor pain of primiparae referring to Hajar Hospital in Shahre Kurd, 2010. J Res Dev Nurs Midw. 2012;9(1):41-50. [View at Publisher] [DOI] [PMID] [Google Scholar]
21. Dadshahi S, Torkzahrani S, Janati-Ataie P, Nasiri M. Does continuous labor support by midwife make a difference in delivery outcomes? The Iranian Journal of Obstetrics, Gynecology and Infertility. 2018;20(12):67-76. [View at Publisher] [DOI] [Google Scholar]
22. Bruggemann OM, Parpinelli MA, Osis MJ, Cecatti JG, Neto ASC. Support to woman by a companion of her choice during childbirth: a randomized controlled trial. Reprod Health. 2007;4(1):5. [View at Publisher] [DOI] [PMID] [Google Scholar]
23. Salehi A, Fahami F, Beigi M. The effect of presence of trained husbands beside their wives during childbirth on women's anxiety. Iran J Nurs Midwifery Res. 2016;21(6):611-5. [View at Publisher] [DOI] [PMID] [Google Scholar]
24. Xue WL, He H-G, Chua YJ, Wang W, Shorey S. Factors influencing first-time fathers' involvement in their wives' pregnancy and childbirth: A correlational study. Midwifery. 2018;62:20-8. [View at Publisher] [DOI] [PMID] [Google Scholar]
25. Adeyemi AB, Fatusi AO, Phillips AS, Olajide FO, Awowole IO, Orisawayi AO. Factors associated with the desire for companionship during labor in a Nigerian community. Int J Gynecol Obstet. 2018;141(3):360-5. [View at Publisher] [DOI] [PMID] [Google Scholar]
26. Yeshitila YG, Memah P. Birth preparedness and complication readiness among husbands and its association with skilled birth attendance in southern Ethiopia. BMC Pregnancy Childbirth. 2022;22(1):852. [View at Publisher] [DOI] [PMID] [Google Scholar]
27. Johansson M, Fenwick J, Premberg A. A meta-synthesis of fathers' experiences of their partner's labour and the birth of their baby. Midwifery. 2015;31(1):9-18. [View at Publisher] [DOI] [PMID] [Google Scholar]
28. Xue WL, Shorey S, Wang W, He H-G. Fathers' involvement during pregnancy and childbirth: an integrative literature review. Midwifery. 2018;62:135-45. [View at Publisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
