
Volume 18, Issue 2 (7-2021)
J Res Dev Nurs Midw 2021, 18(2): 21-25 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Puryaghoob M, Doosti Irani M, Masoumi N, Parvizy S. The Effect of Virtual Self-Care Education on the Perception of Type 1 Diabetes-Related Stigma in Female Adolescents with Diabetes: A Clinical Trial. J Res Dev Nurs Midw 2021; 18 (2) :21-25
URL: http://nmj.goums.ac.ir/article-1-1211-en.html
URL: http://nmj.goums.ac.ir/article-1-1211-en.html



1- Department of Medical, Vali-e-Asr Hospital, School of Nursing and Midwifery, Zanjan University of Medical Sciences, Zanjan, Iran
2- Department of Operating Room, School of Nursing and Midwifery, Shahrekord University of Medical Sciences, Shahrekord, Iran
3- Master of Science in Medical-Surgical Nursing, Abhar School of Nursing, Zanjan University of Medical Sciences, Zanjan, Iran
4- Department of Medical Education, School of Medicine, Iran University of Medical Sciences, Tehran, Iran. ,s_parvizy@yahoo.com
2- Department of Operating Room, School of Nursing and Midwifery, Shahrekord University of Medical Sciences, Shahrekord, Iran
3- Master of Science in Medical-Surgical Nursing, Abhar School of Nursing, Zanjan University of Medical Sciences, Zanjan, Iran
4- Department of Medical Education, School of Medicine, Iran University of Medical Sciences, Tehran, Iran. ,
Full-Text [PDF 816 kb]
(1561 Downloads)
| Abstract (HTML) (4373 Views)
Full-Text: (1174 Views)
Highlights:
What is current knowledge?
Given the importance of diabetes-related stigma and its coincidence with adolescence, it is necessary to implement a self-care program to strengthen knowledge, improve attitudes and practice in adolescents.
What is new here?
Self-care education via virtual social networks was effective in reducing the stigma perception.
Introduction
Diabetes is a common chronic disease that is characterized by the impaired metabolisms of carbohydrates, fats, and proteins in addition to the complete or partial defect in insulin secretion in the body (1).
Type 1 diabetes is more common in people under the age of 20 (2). The importance and necessity of controlling diabetes is doubled due to the progressive increase in its prevalence in adolescents (3). Studies have reported the adolescence as the most difficult stage to control and manage type1 diabetes (4). This is due to the higher insulin resistance during puberty (5), not following the treatment (4), and having less desire to continue therapeutic behaviors in comparison to healthy people (6), leading to more complications in them (7). People with diabetes suffer from a variety of physical and psychological complications (4); and stigma is a psychological complication of this disease (8, 9).
The feeling of being stigmatized is a kind of labeling in a way that the person is differentiated from the environment for physical or psychological reasons and is in a state of being stigmatized. This characteristic is a result of the difference between expected norms of the ideal situation and the real situation in a way that a person's identity is degraded from a complete and ordinary person to a stigmatized person (10). The perceived stigma causes embarrassment due to illness or a feeling of guilt due to the lack of prevention (11). From the point of view of ordinary people in society, a person with diabetes seems to be considered a pitiful, always sick, and a rejected person for marriage (6). On the other hand, fear of stigma is a major obstacle in the treatment of diabetes that exacerbates the complications of diabetes (7, 12, and 13) and impose suffering and high costs (14) because stigma and discrimination may lead to social isolation and low self-esteem in diabetics. This effect is higher in all aspects of adolescent girls' lives, affecting their maturity and emotional performance (15).
Studies indicate that the stigma in patients with diabetes leads to poor attitudes towards the self-care behaviors (16). Unfortunately, despite the costs for preventing and controlling diabetes and its complications, the numbers of people with diabetes and its physical and psychological complications, especially stigma, are increasing every day (8) probably due to the weakness of self-care behaviors (17).
Self-care refers to the correct and timely injection of insulin, adherence to diet, proper physical activity, and the ability to recognize the symptoms of hyperglycemia (18). If the nurses' educational interventions for issues such as self-care to control diabetes are implemented via the Internet, computers, and popular social networks (19) in Iran (20), the adolescents can be inadvertently pushed into the path of disease control in cyberspace (21). Despite various studies on the effect of education via the cyberspace and group sessions on other disease-related stigma (22-24), there was no relevant study on the diabetic patients.
Cyberspace is a powerful tool for educating patients to overcome stigma due to its attractiveness and ease of use. Social networks provide an appropriate platform for people with diabetes to not only exchange information, but also support each other (25). Telegram is a highly popular social network in Iran (26). Despite the existence of such a powerful educational platform and the effects of peer groups in reducing stigma, unfortunately there is no necessary measure in this field in the Iranian health care system and no suitable platform for diabetics to communicate with each other.
Given the importance of diabetes-dependent stigma and the need to implement an available self-care program to strengthen the adolescents' knowledge, the present study aimed to determine the effect of virtual self-care education on type1 diabetes-related stigma in the adolescent girls.
Methods
The present quasi-experimental clinical trial studied the adolescent girls who visited the Iranian Diabetes Society (IDS) in Tehran during May to July 2016. Inclusion criteria: age 14-18 years; diagnosis of type 1 diabetes by a physician; at least six months after the diagnosis; having a non-damaged mobile phone with the ability to install Telegram program; and not suffering from any chronic debilitating disease rather than diabetes. Exclusion criteria: withdrawal from the study; hospitalization; and cell phone failure during the study (Figure 1).
The sample size was calculated to be 76 to reach at least 80% of the test power to detect a significant difference of less than 0.05 between groups based on similar studies (27, 28) with a standard deviation of 4.7. According to the 15% probability of sample loss, the sample size of 45 was estimated in each experimental and control group.

In the present study, we utilized a demographic questionnaire, including age, education level, duration of disease, family history of diabetes, and duration of using social networks, and also a type 1 diabetes-related stigma questionnaire to examine the data. The questionnaire was designed by Doosti Irani (2014) and its validity and reliability were reviewed by the author, and its alpha coefficient was calculated to be 0.938. The questionnaire had 35 five-point Likert questions each of which was scored from 1 to 5 according to one of five options, "strongly agree, agree, neutral, disagree, and strongly disagree", respectively. The minimum score of the questionnaire was 35, and the maximum was 175. A higher score indicated a greater perception of stigma (29).
We collected the samples using the convenience sampling method. Therefore, a list of names and telephone numbers of 180 parents of adolescents with type 1 diabetes, who met the inclusion criteria, were obtained from the management of the Iranian Diabetes Society, and the informed written consent was obtained from 100 parents after contacting them by phone and explaining the study process by the researcher. After receiving the adolescents' phone numbers from their parents, they were contacted and explained about the study process and purpose. Ten adolescents were excluded due to lack of consent and interest in participating in the study. A total of 90 individuals were randomly assigned to the experimental (n=45) and control (n=45) groups using two white and red balls. Two separate groups were established on Telegram under the researcher's management; and the experimental and control group individuals became members of the groups.
The researcher sent the demographic information and type 1 diabetes-related stigma perception questionnaires to each adolescent via the Telegram social network to respond to them.
Therefore, the amount of type 1 diabetes-related stigma was first measured in the participants before the intervention, and the results indicated some degrees of disease-related stigma in the individuals.
The researcher shared 1 message per day from the collection of self-care education messages in text and video attachments relating to the principles of type 1 diabetes self-care in diet, physical activity, blood sugar self-monitoring, insulin injection, insulin unit dose and absorption speed adjustment in the experimental group on the Telegram social network for 12 weeks. He also shared a message (1 message per day) without the content of self-care education in social, scientific, and cultural fields in the control group on the Telegram social network for 12 weeks.
In order to approve the educational content by the experts, it was given to a number of adolescents with diabetes at different ages to comment on it so that we could identify its strengths and weaknesses. After collecting their comments, the self-care content was developed based on what adolescents with type 1 diabetes should know, and its validation was done based on the approval of experts and professors. It was done by nine faculty members of the School of Nursing and Midwifery of Iran University of Medical Sciences and a faculty member of the School of Nursing and Midwifery of Shahrekord University of Medical Sciences.
It should be noted that the messages were presented interactively in both groups and the members gave feedback to it; and the individuals in both experimental and control groups did not know each other. After completing the study, the content of self-care education was provided for the control group.
Individuals in both groups were able to provide suggestions and comments, and ask questions about the messages in the group so that the group members could exchange ideas and they could be answered by the researcher as the group manager.
The time of the last visit of both groups was controlled by the researcher. The individuals, who were not online for at least seven days and did not see the messages or did not have any feedback, were first contacted by text messages, and if not answered, by phone call and they asked their cause to receive another mobile number from them and send the messages to the new numbers. Immediately and four weeks after the intervention, the type 1 diabetes-related stigma questionnaire was sent to each individual on Telegram to be responded. Data were presented using descriptive statistic, including mean and standard deviation or frequency and proportions. To comparison of categorical variable and continues variable in interventional and control group were used the chi-square test and independent t-test, respectively. Also, repeated measures ANOVA were used in order to examine possible variations between group in time. In other to analyzing the data, SPSS Statistics for Windows, version 16 (SPSS Inc., Chicago, Ill., USA). Results
Results
The results indicated that the mean age of patients in the intervention and control groups were 15.89 ±1.43 and 15.92±1.57 years, and the mean duration of diabetes was 7.18±4.10 and 7.31±3.83 years, respectively.
Collectively, 34.2% of mothers and 52.6% of fathers of participants had high school diploma levels. More than a third of participants used social networks for more than 2 hours a day, and 11 participants used them for less than 30 minutes a day. The comparison of the two groups in terms of demographic variables indicated that the two groups did not differ significantly in terms of variables mentioned in the table such as age, education level, and history of infection (Table 1).
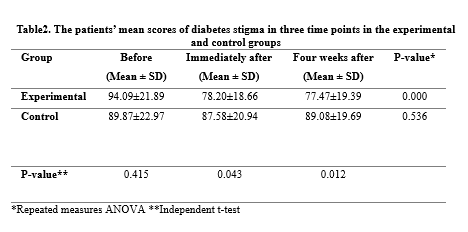
The independent t-test indicated that the mean±standard deviation of the perceived stigma score were not statistically significant between the experimental and control groups before the study (P>0.05).
Findings of repeated measures analysis of variance indicated that the mean stigma scores in the experimental group was different from the others at least at one time (P<0.001).
According to the Bonferroni determination test, there were statistically significant differences in the experimental group between the mean scores of stigma before and immediately after the study (P<0.001) and 4 weeks after the study (P<0.001) so that the mean scores of stigma in the experimental group immediately and 4 weeks after the study decreased by 15.89 and 16.62, respectively. In other words, the mean score of stigma in the experimental group before the study was higher than the other two times and the score of stigma in the experimental group gradually decreased after the study and it was statistically significant. (P<0.05). The results indicated the significant reduction in stigma immediately and 4 weeks after the study compared to the beginning of the study (P<0.05), indicating the effectiveness and permanence of self-care education for the adolescents. The results also indicated that there was no statistically significant difference between the mean scores of stigma in the control group at different times (P=0.536). The mean score of stigma in the control group showed only a reduction of 2.29 immediately after the study or a reduction of 0.79 four weeks after the study (P>0.05) (Table 2). Another finding of the study was the comparison of the perceived stigma score in the experimental and control groups immediately after the study, indicating a statistically significant difference using the independent t-test (P=0.001). In other words, the experimental group showed a greater reduction in stigma than the control group immediately after the study. According to the comparison of the perceived stigma score between the experimental and control groups four weeks after the study, the results indicated a statistically significant difference between the experimental and control groups (P=0.001) (Table 2).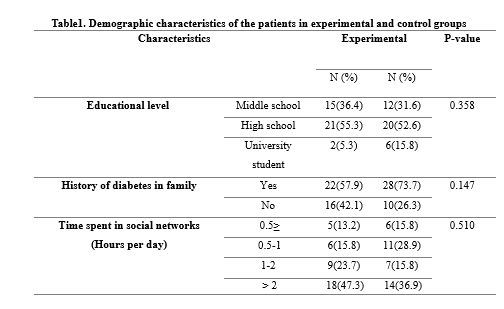
 Discussion
Discussion
The results of the present study indicated that the self-care education via virtual social networks was effective in reducing the perception of type 1 diabetes-related stigma. Furthermore, effective results can be achieved by providing self-care education and its continuation.
According to the results, the participants had some degrees of type 1 diabetes-related stigma, indicating the general prevalence of stigma among the participants. The present findings were consistent with results of studies by Wakawa (2014), Abdoli (2013), and Browne (2013).
Another result of the present study was the statistically significant difference of the experimental and control groups in terms of stigma scores immediately after the study (P=0.001). The perceived stigma scores were also statistically significant between the experimental and control groups four weeks after the study. (P= 0.001)
The results of a study by Barroso were consistent with the present results. In Barroso's study, a 45-minute video containing the problems and the way of resolving them was displayed for people with HIV and immunodeficiency in the experimental group for 4 weeks (once a week) and continued for 12 weeks. The disease-related stigma levels were significantly lower at 4 and 16 weeks after the study compared to the beginning of the study; and the stigma levels were statistically and significantly different at 4 and 16 weeks after the study (24). Finkelstein also achieved similar results to the present study. Performing an educational intervention in 2 sessions, Finkelstein reported a significant reduction in the amount of disease-related stigma immediately and 6 months after the education period in comparison with before the study and the control group (30), but some studies achieved inconsistent results with the present results. In Corrigan's study, the mean scores of the disease-related stigma were measured in the experimental and control groups immediately after two education sessions and a week after the intervention (with the content of schizophrenia), but no statistically significant difference was found between the experimental and control groups (31). According to studies by Kiropoulos and Yanos, who included the 3-month and 1-week follow-up respectively, the mean scores of disease-related stigma were not statistically significant compared to before and immediately after the study (22, 23). Kiropoulos considered the lack of an education method to reduce disease-related stigma and the short follow-up time as possible reasons for the results of his study (23) and Yanos attributed the slight change in the stigma of the intervention group to the small number of samples and their intermittent loss due to fluctuations in their depression that limited the researcher's ability to determine the effect of educational intervention (22). Despite the provision of education by videotape, websites, and face-to-face methods about the disease-related topics and ways to reduce disease-related stigma in the above studies, their results did not show any positive effect of the methods on reducing stigma.
Given that the type and prevalence of diseases are serious factors affecting the incidence of disease-related stigma and also the prevailing atmosphere; and cultural characteristics of the society also affect the occurrence and increase of disease-related stigma (32), the cause of different results of the present study with the results of studies by Corrigan, Kiropoulos, and Yanos can be attributed to difference in the type of disease and cultural characteristics of the research environments. A change in content or the simultaneous implementation of several educational interventions may be necessary to make significant changes in the degree of stigma relating to mental diseases such as schizophrenia and depression.
A main limitation of the present study was the relationship between individuals in the control and experimental groups, which despite the recommendations and rules for the samples, might still occur in several cases. Another limitation of the study was the possibility of permanent filtering of some social networks in Iran; hence, we suggest the use of a native social network.
Conclusion
The knowledge about the health-promoting behaviors is an important principle for the success of a person's with diabetes in self-care because adherence to self-care behaviors is the first step towards helping the patients better care and manage their diseases; hence, a significant reduction in the disease-related stigma 4 weeks after the end of the education period compared to before the study in the experimental group and in comparison with the control group in the present study indicated the effective virtual education on data retention and stability up to a month after the study. In general, the more the education is separated from the traditional method of lecturing and is accompanied by attractive and popular methods such as social networks, the more it improves the level of learning and makes it more enjoyable. Since the feeling of disease-related stigma is related to the individuals, on the one hand, and the society on the other hand, if education is done at both individual and community levels, we can expect its greater impact on reducing the disease-related stigma.
Acknowledgements
The present study was derived from a master's thesis at Iran University of Medical Sciences. We are grateful to the research deputy of Iran University of Medical Sciences and also all the staff of the Iranian Diabetes Society (IDS), Dr. Rajab, the esteemed principal of IDS, and all patients who cooperated in the research.
Funding source
This research received a research grant from the research deputy of Iran University of Medical Sciences.
Ethical statement
The study was approved by the Health Research Ethics Committee of Iran University of Medical Sciences (Code: IR.IUMS.REC.1394.9311687001). Also registration in Iranian Registry of Clinical Trials (code: IRCT201511197101N3).
Conflict of interest
The authors declare that there is no conflict of interest.
performed the data collection; MDI and NM performed the data analysis; MP,
MDI, and SP were responsible for the drafting of the manuscript.
What is current knowledge?
Given the importance of diabetes-related stigma and its coincidence with adolescence, it is necessary to implement a self-care program to strengthen knowledge, improve attitudes and practice in adolescents.
What is new here?
Self-care education via virtual social networks was effective in reducing the stigma perception.
Introduction
Diabetes is a common chronic disease that is characterized by the impaired metabolisms of carbohydrates, fats, and proteins in addition to the complete or partial defect in insulin secretion in the body (1).
Type 1 diabetes is more common in people under the age of 20 (2). The importance and necessity of controlling diabetes is doubled due to the progressive increase in its prevalence in adolescents (3). Studies have reported the adolescence as the most difficult stage to control and manage type1 diabetes (4). This is due to the higher insulin resistance during puberty (5), not following the treatment (4), and having less desire to continue therapeutic behaviors in comparison to healthy people (6), leading to more complications in them (7). People with diabetes suffer from a variety of physical and psychological complications (4); and stigma is a psychological complication of this disease (8, 9).
The feeling of being stigmatized is a kind of labeling in a way that the person is differentiated from the environment for physical or psychological reasons and is in a state of being stigmatized. This characteristic is a result of the difference between expected norms of the ideal situation and the real situation in a way that a person's identity is degraded from a complete and ordinary person to a stigmatized person (10). The perceived stigma causes embarrassment due to illness or a feeling of guilt due to the lack of prevention (11). From the point of view of ordinary people in society, a person with diabetes seems to be considered a pitiful, always sick, and a rejected person for marriage (6). On the other hand, fear of stigma is a major obstacle in the treatment of diabetes that exacerbates the complications of diabetes (7, 12, and 13) and impose suffering and high costs (14) because stigma and discrimination may lead to social isolation and low self-esteem in diabetics. This effect is higher in all aspects of adolescent girls' lives, affecting their maturity and emotional performance (15).
Studies indicate that the stigma in patients with diabetes leads to poor attitudes towards the self-care behaviors (16). Unfortunately, despite the costs for preventing and controlling diabetes and its complications, the numbers of people with diabetes and its physical and psychological complications, especially stigma, are increasing every day (8) probably due to the weakness of self-care behaviors (17).
Self-care refers to the correct and timely injection of insulin, adherence to diet, proper physical activity, and the ability to recognize the symptoms of hyperglycemia (18). If the nurses' educational interventions for issues such as self-care to control diabetes are implemented via the Internet, computers, and popular social networks (19) in Iran (20), the adolescents can be inadvertently pushed into the path of disease control in cyberspace (21). Despite various studies on the effect of education via the cyberspace and group sessions on other disease-related stigma (22-24), there was no relevant study on the diabetic patients.
Cyberspace is a powerful tool for educating patients to overcome stigma due to its attractiveness and ease of use. Social networks provide an appropriate platform for people with diabetes to not only exchange information, but also support each other (25). Telegram is a highly popular social network in Iran (26). Despite the existence of such a powerful educational platform and the effects of peer groups in reducing stigma, unfortunately there is no necessary measure in this field in the Iranian health care system and no suitable platform for diabetics to communicate with each other.
Given the importance of diabetes-dependent stigma and the need to implement an available self-care program to strengthen the adolescents' knowledge, the present study aimed to determine the effect of virtual self-care education on type1 diabetes-related stigma in the adolescent girls.
Methods
The present quasi-experimental clinical trial studied the adolescent girls who visited the Iranian Diabetes Society (IDS) in Tehran during May to July 2016. Inclusion criteria: age 14-18 years; diagnosis of type 1 diabetes by a physician; at least six months after the diagnosis; having a non-damaged mobile phone with the ability to install Telegram program; and not suffering from any chronic debilitating disease rather than diabetes. Exclusion criteria: withdrawal from the study; hospitalization; and cell phone failure during the study (Figure 1).
The sample size was calculated to be 76 to reach at least 80% of the test power to detect a significant difference of less than 0.05 between groups based on similar studies (27, 28) with a standard deviation of 4.7. According to the 15% probability of sample loss, the sample size of 45 was estimated in each experimental and control group.
In the present study, we utilized a demographic questionnaire, including age, education level, duration of disease, family history of diabetes, and duration of using social networks, and also a type 1 diabetes-related stigma questionnaire to examine the data. The questionnaire was designed by Doosti Irani (2014) and its validity and reliability were reviewed by the author, and its alpha coefficient was calculated to be 0.938. The questionnaire had 35 five-point Likert questions each of which was scored from 1 to 5 according to one of five options, "strongly agree, agree, neutral, disagree, and strongly disagree", respectively. The minimum score of the questionnaire was 35, and the maximum was 175. A higher score indicated a greater perception of stigma (29).
We collected the samples using the convenience sampling method. Therefore, a list of names and telephone numbers of 180 parents of adolescents with type 1 diabetes, who met the inclusion criteria, were obtained from the management of the Iranian Diabetes Society, and the informed written consent was obtained from 100 parents after contacting them by phone and explaining the study process by the researcher. After receiving the adolescents' phone numbers from their parents, they were contacted and explained about the study process and purpose. Ten adolescents were excluded due to lack of consent and interest in participating in the study. A total of 90 individuals were randomly assigned to the experimental (n=45) and control (n=45) groups using two white and red balls. Two separate groups were established on Telegram under the researcher's management; and the experimental and control group individuals became members of the groups.
The researcher sent the demographic information and type 1 diabetes-related stigma perception questionnaires to each adolescent via the Telegram social network to respond to them.
Therefore, the amount of type 1 diabetes-related stigma was first measured in the participants before the intervention, and the results indicated some degrees of disease-related stigma in the individuals.
The researcher shared 1 message per day from the collection of self-care education messages in text and video attachments relating to the principles of type 1 diabetes self-care in diet, physical activity, blood sugar self-monitoring, insulin injection, insulin unit dose and absorption speed adjustment in the experimental group on the Telegram social network for 12 weeks. He also shared a message (1 message per day) without the content of self-care education in social, scientific, and cultural fields in the control group on the Telegram social network for 12 weeks.
In order to approve the educational content by the experts, it was given to a number of adolescents with diabetes at different ages to comment on it so that we could identify its strengths and weaknesses. After collecting their comments, the self-care content was developed based on what adolescents with type 1 diabetes should know, and its validation was done based on the approval of experts and professors. It was done by nine faculty members of the School of Nursing and Midwifery of Iran University of Medical Sciences and a faculty member of the School of Nursing and Midwifery of Shahrekord University of Medical Sciences.
It should be noted that the messages were presented interactively in both groups and the members gave feedback to it; and the individuals in both experimental and control groups did not know each other. After completing the study, the content of self-care education was provided for the control group.
Individuals in both groups were able to provide suggestions and comments, and ask questions about the messages in the group so that the group members could exchange ideas and they could be answered by the researcher as the group manager.
The time of the last visit of both groups was controlled by the researcher. The individuals, who were not online for at least seven days and did not see the messages or did not have any feedback, were first contacted by text messages, and if not answered, by phone call and they asked their cause to receive another mobile number from them and send the messages to the new numbers. Immediately and four weeks after the intervention, the type 1 diabetes-related stigma questionnaire was sent to each individual on Telegram to be responded. Data were presented using descriptive statistic, including mean and standard deviation or frequency and proportions. To comparison of categorical variable and continues variable in interventional and control group were used the chi-square test and independent t-test, respectively. Also, repeated measures ANOVA were used in order to examine possible variations between group in time. In other to analyzing the data, SPSS Statistics for Windows, version 16 (SPSS Inc., Chicago, Ill., USA).
The results indicated that the mean age of patients in the intervention and control groups were 15.89 ±1.43 and 15.92±1.57 years, and the mean duration of diabetes was 7.18±4.10 and 7.31±3.83 years, respectively.
Collectively, 34.2% of mothers and 52.6% of fathers of participants had high school diploma levels. More than a third of participants used social networks for more than 2 hours a day, and 11 participants used them for less than 30 minutes a day. The comparison of the two groups in terms of demographic variables indicated that the two groups did not differ significantly in terms of variables mentioned in the table such as age, education level, and history of infection (Table 1).
The independent t-test indicated that the mean±standard deviation of the perceived stigma score were not statistically significant between the experimental and control groups before the study (P>0.05).
Findings of repeated measures analysis of variance indicated that the mean stigma scores in the experimental group was different from the others at least at one time (P<0.001).
According to the Bonferroni determination test, there were statistically significant differences in the experimental group between the mean scores of stigma before and immediately after the study (P<0.001) and 4 weeks after the study (P<0.001) so that the mean scores of stigma in the experimental group immediately and 4 weeks after the study decreased by 15.89 and 16.62, respectively. In other words, the mean score of stigma in the experimental group before the study was higher than the other two times and the score of stigma in the experimental group gradually decreased after the study and it was statistically significant. (P<0.05). The results indicated the significant reduction in stigma immediately and 4 weeks after the study compared to the beginning of the study (P<0.05), indicating the effectiveness and permanence of self-care education for the adolescents. The results also indicated that there was no statistically significant difference between the mean scores of stigma in the control group at different times (P=0.536). The mean score of stigma in the control group showed only a reduction of 2.29 immediately after the study or a reduction of 0.79 four weeks after the study (P>0.05) (Table 2). Another finding of the study was the comparison of the perceived stigma score in the experimental and control groups immediately after the study, indicating a statistically significant difference using the independent t-test (P=0.001). In other words, the experimental group showed a greater reduction in stigma than the control group immediately after the study. According to the comparison of the perceived stigma score between the experimental and control groups four weeks after the study, the results indicated a statistically significant difference between the experimental and control groups (P=0.001) (Table 2).
The results of the present study indicated that the self-care education via virtual social networks was effective in reducing the perception of type 1 diabetes-related stigma. Furthermore, effective results can be achieved by providing self-care education and its continuation.
According to the results, the participants had some degrees of type 1 diabetes-related stigma, indicating the general prevalence of stigma among the participants. The present findings were consistent with results of studies by Wakawa (2014), Abdoli (2013), and Browne (2013).
Another result of the present study was the statistically significant difference of the experimental and control groups in terms of stigma scores immediately after the study (P=0.001). The perceived stigma scores were also statistically significant between the experimental and control groups four weeks after the study. (P= 0.001)
The results of a study by Barroso were consistent with the present results. In Barroso's study, a 45-minute video containing the problems and the way of resolving them was displayed for people with HIV and immunodeficiency in the experimental group for 4 weeks (once a week) and continued for 12 weeks. The disease-related stigma levels were significantly lower at 4 and 16 weeks after the study compared to the beginning of the study; and the stigma levels were statistically and significantly different at 4 and 16 weeks after the study (24). Finkelstein also achieved similar results to the present study. Performing an educational intervention in 2 sessions, Finkelstein reported a significant reduction in the amount of disease-related stigma immediately and 6 months after the education period in comparison with before the study and the control group (30), but some studies achieved inconsistent results with the present results. In Corrigan's study, the mean scores of the disease-related stigma were measured in the experimental and control groups immediately after two education sessions and a week after the intervention (with the content of schizophrenia), but no statistically significant difference was found between the experimental and control groups (31). According to studies by Kiropoulos and Yanos, who included the 3-month and 1-week follow-up respectively, the mean scores of disease-related stigma were not statistically significant compared to before and immediately after the study (22, 23). Kiropoulos considered the lack of an education method to reduce disease-related stigma and the short follow-up time as possible reasons for the results of his study (23) and Yanos attributed the slight change in the stigma of the intervention group to the small number of samples and their intermittent loss due to fluctuations in their depression that limited the researcher's ability to determine the effect of educational intervention (22). Despite the provision of education by videotape, websites, and face-to-face methods about the disease-related topics and ways to reduce disease-related stigma in the above studies, their results did not show any positive effect of the methods on reducing stigma.
Given that the type and prevalence of diseases are serious factors affecting the incidence of disease-related stigma and also the prevailing atmosphere; and cultural characteristics of the society also affect the occurrence and increase of disease-related stigma (32), the cause of different results of the present study with the results of studies by Corrigan, Kiropoulos, and Yanos can be attributed to difference in the type of disease and cultural characteristics of the research environments. A change in content or the simultaneous implementation of several educational interventions may be necessary to make significant changes in the degree of stigma relating to mental diseases such as schizophrenia and depression.
A main limitation of the present study was the relationship between individuals in the control and experimental groups, which despite the recommendations and rules for the samples, might still occur in several cases. Another limitation of the study was the possibility of permanent filtering of some social networks in Iran; hence, we suggest the use of a native social network.
Conclusion
The knowledge about the health-promoting behaviors is an important principle for the success of a person's with diabetes in self-care because adherence to self-care behaviors is the first step towards helping the patients better care and manage their diseases; hence, a significant reduction in the disease-related stigma 4 weeks after the end of the education period compared to before the study in the experimental group and in comparison with the control group in the present study indicated the effective virtual education on data retention and stability up to a month after the study. In general, the more the education is separated from the traditional method of lecturing and is accompanied by attractive and popular methods such as social networks, the more it improves the level of learning and makes it more enjoyable. Since the feeling of disease-related stigma is related to the individuals, on the one hand, and the society on the other hand, if education is done at both individual and community levels, we can expect its greater impact on reducing the disease-related stigma.
Acknowledgements
The present study was derived from a master's thesis at Iran University of Medical Sciences. We are grateful to the research deputy of Iran University of Medical Sciences and also all the staff of the Iranian Diabetes Society (IDS), Dr. Rajab, the esteemed principal of IDS, and all patients who cooperated in the research.
Funding source
This research received a research grant from the research deputy of Iran University of Medical Sciences.
Ethical statement
The study was approved by the Health Research Ethics Committee of Iran University of Medical Sciences (Code: IR.IUMS.REC.1394.9311687001). Also registration in Iranian Registry of Clinical Trials (code: IRCT201511197101N3).
Conflict of interest
The authors declare that there is no conflict of interest.
Author contributions
MP and SP were responsible for the study conception and design; MPperformed the data collection; MDI and NM performed the data analysis; MP,
MDI, and SP were responsible for the drafting of the manuscript.
Type of study: Original Article |
Subject:
Nursing
References
1. Barnard KD, Lloyd CE, Holt RI. Psychological burden of diabetes and what it means to people with diabetes. Psychol Diabetes Care. 2012; 2:1-22. [View at paplisher] [DOI] [Google Scholar]
2. Melmed S, Polonsky KS, Larsen PR, Kronenberg HM. Williams textbook of endocrinology. Elsevier Health Sciences; 2015. [View at paplisher] [Google Scholar]
3. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87(1):4-14. [View at paplisher] [DOI] [PMID] [Google Scholar]
4. Kermansaravi F, Navidian A, Ansarymoghadam A. Quality of Life in Type 1 Diabetic Adolescents in Zahedan (2011). IJEM. 2012; 13(6):651-657. [Persian] [View at paplisher] [Google Scholar]
5. Rezasefat Balesbaneh A, Mirhaghjou N, Jafsri Asl M, Kohmanaee S, Kazemnejad Leili E, Monfared A. Correlation between self-care and self-efficacy in adolescents with type 1 diabetes. J Holist Nurs Midwifery. 2014; 24 (2) :18-24 [Persian] [View at paplisher] [Google Scholar]
6. Abdoli S, Doosti Irani M, Parvizi S, Seyed Fatemi N, Amini M. Living in the shadow and light: Iranian youths' responses to diabetes-related stigma. EOJNSS. 2013;2(2s):439-48. [View at paplisher] [DOI] [Google Scholar]
7. Børte S, Ottersen VS. Stigmatization of children with chronic diseases, exemplified by type 1 diabetes mellitus.: Differences between India and Norway 2012. [View at paplisher] [Google Scholar]
8. Liu NF, Brown AS, Folias AE, Younge MF, Guzman SJ, Close KL, et al. Stigma in people with type 1 or type 2 diabetes. Clin Diabetes. 2017;35(1):27-34. [View at paplisher] [DOI] [PMID] [Google Scholar]
9. Brazeau A, Nakhla M, Wright M, Henderson M, Panagiotopoulos C, Pacaud D, Et Al. Stigma and Its Association with Glycemic Control and Hypoglycemia in Adolescents and Young Adults with Type 1 Diabetes: Cross-Sectional Study. J Med Internet Res. 2018; 20(4): e151. [View at paplisher] [DOI] [PMID] [Google Scholar]
10. Abdoli S, Abazari P, Mardanian L. Exploring diabetes type 1-related stigma. Iran J Nurs Midwifery Res. 2013; 18(1):65. [View at paplisher] [Google Scholar]
11. Earnshaw VA, Quinn DM. The impact of stigma in healthcare on people living with chronic illnesses. Journal of Health Psychology. 2012;17(2):157-68. [View at paplisher] [DOI] [PMID] [Google Scholar]
12. shirazi M, anoosheh M, rajab A. The effect of self-care program education by group discussion method on self-concept in diabetic adolescent girls reffered to Iranian Diabetes Society. IJNR. 2011; 6 (22) :40-52. [Persian] [View at paplisher] [Google Scholar]
13. Abdoli S, As-hktorab T, Ahmadi F, Parvizy S, Dunning T. Seeking new identity through the empowerment process. IUMS. 2014;19(2):145-151. [Persian] [View at paplisher] [Google Scholar]
14. Ahmadi A, Hasanzadeh J, Rahimi Madiseh M, Lashkari L. Effective Factors In The Quality Of Life In Patients With Type 2 Diabetes In Chaharmahal & Bakhteyari Province. Journal of north Khorasan University of Medical Sciences. 2011;3(17). [Persian] [View at paplisher] [DOI] [Google Scholar]
15. Ahmadi F, Hemati Maslak Pak M, Anoush M, Hajizadeh E, Rajab A. Diabetic adolescent girls perspective on marriage: a qualitative study. JFR.2010; 5(20):455-465. [Persian] [View at paplisher] [Google Scholar]
16. Kato A, Fujimaki Y, Fujimori S, Isogawa A, Onishi Y, Suzuki R, et al. Association between self-stigma and self-care behaviors in patients with type 2 diabetes: a cross-sectional study. BMJ Open Diabetes Res Care. 2016;4(1): e000156. [View at paplisher] [DOI] [PMID] [Google Scholar]
17. Yeganeh A, AhmadzadehHeshmat A. Quality of life of diabetic patients with lower extremity amputation. JMUMS. 2014;24(116):93-101. [Persian] [View at paplisher] [Google Scholar]
18. Khezerloo S, Feizi A. A Survey Of Relationship Between Perceived Selfefficacy And Self-Care Performance In Diabetic Patients Referring To Urmia Diabetes Center. Nurs Midwifery J. 2012; 10(3):369-75. [Persian] [View at paplisher] [Google Scholar]
19. Shirazi M, Anoosheh M, Rajab A. The effect of self-care program education through group discussion method on knowledge and practice in diabetic adolescent girls referring to Iranian Diabetes Society. Iranian Journal of Medical Education. 2011;10(5):982-93. [Persian] [View at paplisher] [Google Scholar]
20. borhani F. The effect of empowerment program on hemoglobin A1C in type 2 diabetes patients. Med Surg Nurs J. 2013; 1(2): e87580. [Persian] [View at paplisher] [Google Scholar]
21. Lee MK. Effects of mobile phone-based app learning compared to computer-based web learning on nursing students: pilot randomized controlled trial. Healthc Inform Res. 2015; 21(2):125-33.
https://doi.org/10.4258/hir.2015.21.2.125 [View at paplisher] [DOI] [PMID] [Google Scholar]
22. Yanos PT, Roe D, West ML, Smith SM, Lysaker PH. Group-based treatment for internalized stigma among persons with severe mental illness: Findings from a randomized controlled trial. Psychol Serv. 2012; 9(3):248-258. [View at paplisher] [DOI] [PMID] [Google Scholar]
23. Kiropoulos LA, Griffiths KM, Blashki G. Effects of a multilingual information website intervention on the levels of depression literacy and depression-related stigma in Greek-born and Italian-born immigrants living in Australia: a randomized controlled trial. J Med Internet Res. 2011; 13(2). [View at paplisher] [DOI] [PMID] [Google Scholar]
24. Barroso J, Relf MV, Williams MS, Arscott J, Moore ED, Caiola C, et al. A randomized controlled trial of the efficacy of a stigma reduction intervention for HIV-infected women in the Deep South. AIDS patient care STDS. 2014; 28(9):489-98. [View at paplisher] [DOI] [PMID] [Google Scholar]
25. Irani MD, Abdoli S, Parvizy S, Fatemi NS, Amini M. Breaking stigma within us: the role of people with type 1 diabetes in overcoming diabetes-related stigma. Int JDiabetes Deve Ctries. 2015; 35(2):264-70. [View at paplisher] [DOI] [Google Scholar]
26. Asnafi AR, Moradi S, Dokhtesmati M, Naeini MP. Using mobile-based social networks by Iranian libraries: The case of Telegram Messenger. Libr Philos Pract. 2017; 2017(1). [View at paplisher] [Google Scholar]
27. Fatusi AO, Hindin MJ. Adolescents and youth in developing countries: Health and development issues in context. J Adolesc. 2010; 33(4):499-508. [View at paplisher] [DOI] [PMID] [Google Scholar]
28. Long KA, Keeley L, Reiter‐Purtill J, Vannatta K, Gerhardt CA, Noll RB. Child‐rearing in the context of childhood cancer: Perspectives of parents and professionals. Pediatric blood & cancer. Pediatr Blood Cancer. 2014; 61(2):326-32. [View at paplisher] [DOI] [PMID] [Google Scholar]
29. Doosti Irani M , Abdoli S, Parvizy S, Seyed Fatemi N. Overcoming diabetes-related stigma in Iran: A participatory action research. Appl Nurs Res. 2017; 36:115-21. [View at paplisher] [DOI] [PMID] [Google Scholar]
30. Finkelstein J, Lapshin O, Wasserman E. Randomized study of different anti-stigma media. Patient Education and Counseling. 2008;71(2):204-14. [View at paplisher] [DOI:10.1016/j.pec.2008.01.002] [PMID] [Google Scholar]
31. Corrigan PW, O'Shaughnessy JR. Changing mental illness stigma as it exists in the real world. Australian Psychologist. 2007;42(2):90-7. [View at paplisher] [DOI] [Google Scholar]
32. Abdoli S, Ashktorab T, Ahmadi F, Parvizi S, Dunning T. The empowerment process in people with Diabetes. an Iranian perspective. Int Nurs Rev. 2008; 55(4):447-453. [View at paplisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
