
Volume 18, Issue 2 (7-2021)
J Res Dev Nurs Midw 2021, 18(2): 29-32 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Seyed Hoshiyar M, Ziaei T, Tatari M, Khoori E. Self-Awareness Counseling on Quality of Life of Menopausal Women. J Res Dev Nurs Midw 2021; 18 (2) :29-32
URL: http://nmj.goums.ac.ir/article-1-1135-en.html
URL: http://nmj.goums.ac.ir/article-1-1135-en.html



1- Golestan University of Medical Sciences, Gorgan, Iran
2- Counselling and Reproductive Health Research Centre, Golestan University of Medical Sciences, Gorgan, Iran
3- Counselling and Reproductive Health Research Centre, Golestan University of Medical Sciences, Gorgan, Iran ,elikami20@yahoo.com
2- Counselling and Reproductive Health Research Centre, Golestan University of Medical Sciences, Gorgan, Iran
3- Counselling and Reproductive Health Research Centre, Golestan University of Medical Sciences, Gorgan, Iran ,
Full-Text [PDF 738 kb]
(1465 Downloads)
| Abstract (HTML) (3574 Views)
Full-Text: (1165 Views)
Highlights:
What is current knowledge?
Counseling, health education and ten core life skills have been able to improve the quality of life of menopausal women by changing their behavior and promoting their health (8- 11), but according to studies, it is not clear which of the ten core life skills have affected the quality of life of menopausal women.
What is new here?
The study findings indicate that the self-awareness group counseling positively affected the quality of life of menopausal women in Gorgan.
Introduction


What is current knowledge?
Counseling, health education and ten core life skills have been able to improve the quality of life of menopausal women by changing their behavior and promoting their health (8- 11), but according to studies, it is not clear which of the ten core life skills have affected the quality of life of menopausal women.
What is new here?
The study findings indicate that the self-awareness group counseling positively affected the quality of life of menopausal women in Gorgan.
Introduction
The basic dimensions of quality of life in the menopause period are generally related to physical, mental and social health (1). The menopausal quality of life refers to a person's perception of a range of health-related symptoms, including hot flashes, night sweats, vaginal dryness, mood disorders, depression, anxiety, low concentration, memory impairment, irritability and sexual dysfunction (2).
Menopause is one of the most important stages of life and the beginning of a new period in women's lives that can be associated with positive, negative and health-threatening features and affect their quality of life(3). Menopausal symptoms and complications including vasomotor, psychological, social, physical and sexual symptoms can reduce the quality of life of women by affecting all aspects of health (4-7).
Although studies indicate that counseling, health education and ten core life skills have been able to improve the quality of life of menopausal women by changing their behavior and promoting their health (8- 11), it is important to note that life skills include several skills and according to their underlying principles, each of which can affect some aspects of quality of life (12). According to studies, it is not clear which of the ten core life skills have affected the quality of life of menopausal women.
Self-awareness plays an important role in promoting mental health and quality of life (13). It can be considered as psychosocial abilities for adaptive and effective behavior (14). People who are more self-aware respond better to life problems by recognizing their characteristics and evaluating beliefs and mental perceptions (15). And they adapt more successfully to their internal and external environment and world general (16).
Menopausal symptoms can cause discomfort, insomnia and low self-esteem (4). High stress, anxiety and depression are also associated with increased severity of menopausal symptoms (17). Since the result of strengthening self-awareness skills are identification and management of emotions, including anger, sadness, stress and the ability to control behavior, increase self-confidence, restore self-esteem and reduce depression (18), it seems that self-awareness can be effective in controlling symptoms and improving the quality of life of menopausal women by addressing various personal and social issues associate with it. Paying attention to menopausal women quality of life and solving their physical, mental and social problems will also be consequently in promoting family health. The present study aimed to determine effect of self-awareness counseling on the menopausal women quality of life in Gorgan, Iran.
Methods
Menopause is one of the most important stages of life and the beginning of a new period in women's lives that can be associated with positive, negative and health-threatening features and affect their quality of life(3). Menopausal symptoms and complications including vasomotor, psychological, social, physical and sexual symptoms can reduce the quality of life of women by affecting all aspects of health (4-7).
Although studies indicate that counseling, health education and ten core life skills have been able to improve the quality of life of menopausal women by changing their behavior and promoting their health (8- 11), it is important to note that life skills include several skills and according to their underlying principles, each of which can affect some aspects of quality of life (12). According to studies, it is not clear which of the ten core life skills have affected the quality of life of menopausal women.
Self-awareness plays an important role in promoting mental health and quality of life (13). It can be considered as psychosocial abilities for adaptive and effective behavior (14). People who are more self-aware respond better to life problems by recognizing their characteristics and evaluating beliefs and mental perceptions (15). And they adapt more successfully to their internal and external environment and world general (16).
Menopausal symptoms can cause discomfort, insomnia and low self-esteem (4). High stress, anxiety and depression are also associated with increased severity of menopausal symptoms (17). Since the result of strengthening self-awareness skills are identification and management of emotions, including anger, sadness, stress and the ability to control behavior, increase self-confidence, restore self-esteem and reduce depression (18), it seems that self-awareness can be effective in controlling symptoms and improving the quality of life of menopausal women by addressing various personal and social issues associate with it. Paying attention to menopausal women quality of life and solving their physical, mental and social problems will also be consequently in promoting family health. The present study aimed to determine effect of self-awareness counseling on the menopausal women quality of life in Gorgan, Iran.
The present clinical trial was carried out on menopausal women who were referred to health centers in Gorgan, Iran in 2018. Sample size of 52 was calculated at 95% confidence level, test power of 80% and loss of 15%, using the formula for determining the sample size of interventional studies (9). The sampling method was stratified random sampling with proportional allocation. First, four health centers were selected from six Gorgan urban health centers by simple random sampling (draw). After identifying 237 menopausal women aged 45-55 years who were one to five years after menopause (according to the Nab electronic system), women were selected by stratified sampling from each health center. Inclusion criteria were having physiological menopause (without medication and surgery), minimum literacy, Iranian nationality, Fars ethnicity, married and living with her spouse, no drug addiction, no hormone therapy in the last six months and no psychiatric illness under treatment. Of 237 menopausal women, 103 did not meet the inclusion criteria and 10 did not willing to participate. Subjects were randomly selected from the remaining 124 individuals and then divided into an intervention (n=26) and a control group (n=26). Written informed consent was taken from all subjects after explaining the research objectives and ensuring confidentiality of personal information.
To prevent possible exchange of information between the control group and the intervention, first the subjects in the control group completed a demographic characteristics form and the Menopause-specific Quality Of Life (MENQOL) questionnaire at baseline, six weeks and 10 weeks after the first time. After the control group samples were completed, the mentioned forms were completed by the intervention group (at baseline), then the women in the intervention group participated in six 45-60-minute weekly group sessions of self-awareness-based counseling using a cognitive-behavioral therapy approach.
Content and structure of the sessions were based on principles of group cognitive therapy (19). At the end of the counseling sessions, and one month the last session, the women of the intervention group completed the MENQOL questionnaire again (Table 1)
To prevent possible exchange of information between the control group and the intervention, first the subjects in the control group completed a demographic characteristics form and the Menopause-specific Quality Of Life (MENQOL) questionnaire at baseline, six weeks and 10 weeks after the first time. After the control group samples were completed, the mentioned forms were completed by the intervention group (at baseline), then the women in the intervention group participated in six 45-60-minute weekly group sessions of self-awareness-based counseling using a cognitive-behavioral therapy approach.
Content and structure of the sessions were based on principles of group cognitive therapy (19). At the end of the counseling sessions, and one month the last session, the women of the intervention group completed the MENQOL questionnaire again (Table 1)
The MENQOL questionnaire was first developed by Hilditch in 1996, and Fallahzadeh et al. (2011) in Iran confirmed its validity and reported its reliability by obtaining a Cronbach's alpha of 0.85 (2). The questionnaire includes 29 questions about symptoms and complications of menopause under four domains: vasomotor (3 questions), psychosocial (7 questions), and physical (16 questions) and sexual (3 questions). Answers are scored based on a Likert scale (point 1 for minimum severity and point 6 for maximum severity). A total score of MENQOL is 0-174. The highest score in all and every domain indicates the inappropriate quality of menopausal life and the lowest score indicates the appropriate quality of menopausal life. Accordingly, in terms of menopausal quality of life, women are divided into three categories: appropriate (score 0-58), moderate (score 59-116) and inappropriate (score 117-174).
Data were analyzed using SPSS Statistics for Windows, version 16 (SPSS Inc., Chicago, Ill., USA). Means and standard deviation, the Chi-square test, independent t-test, Mann-Whitney U test, repeated measures analysis of variance (ANOVA), Friedman test, Bonferroni test and Wilcoxon test were used. A p-value of <0.05 was considered significant.
Results
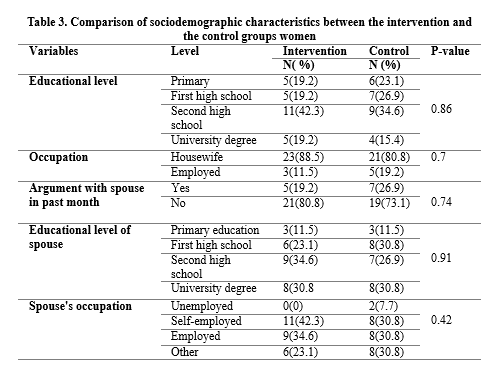
Demographic variables did not differ significantly between the study groups before intervention. In other words, the two groups did not differ in terms of the variables that can affect the menopausal quality of life (Tables 2 and 3).
Data were analyzed using SPSS Statistics for Windows, version 16 (SPSS Inc., Chicago, Ill., USA). Means and standard deviation, the Chi-square test, independent t-test, Mann-Whitney U test, repeated measures analysis of variance (ANOVA), Friedman test, Bonferroni test and Wilcoxon test were used. A p-value of <0.05 was considered significant.
Results
Demographic variables did not differ significantly between the study groups before intervention. In other words, the two groups did not differ in terms of the variables that can affect the menopausal quality of life (Tables 2 and 3).
Except for the total mean score of menopausal quality life and its physical domain, there was no statistically significant difference in terms of other domains of quality of life during menopause between the two groups at baseline. Accordingly, we used the analysis of covariance to adjust the scores of the two variables (menopausal quality life and physical domain). The mean score of menopausal quality of life and physical domain showed a statistically significant difference between the intervention and control groups immediately and a month after the intervention (P=0.001) (Table 4).
To examine the variables of menopausal quality of life, physical, vasomotor and psychosocial domains at three times, according to the assumption of normality, repeated measures ANOVA was performed. The test indicated that in the intervention group the mean score of menopausal quality of life and its physical, psychosocial and sexual domains differed significantly immediately and one month after the intervention compared with baseline.
In vasomotor domain of the intervention group in three times, the results showed that there was no statistically significant difference between mean score of vasomotor domains at baseline and immediately after the intervention. However, the mean score of this domain changed significantly one month after the intervention to baseline and between immediately and one month after intervention.
The mean scores of the mentioned variables in the control group did not change significantly in three times. In comparison between study groups, except for the psychosocial domain, the mean scores of menopausal quality of life and its different domains differed significantly between the study groups one month after the intervention (Table 4).
To examine the variables of menopausal quality of life, physical, vasomotor and psychosocial domains at three times, according to the assumption of normality, repeated measures ANOVA was performed. The test indicated that in the intervention group the mean score of menopausal quality of life and its physical, psychosocial and sexual domains differed significantly immediately and one month after the intervention compared with baseline.
In vasomotor domain of the intervention group in three times, the results showed that there was no statistically significant difference between mean score of vasomotor domains at baseline and immediately after the intervention. However, the mean score of this domain changed significantly one month after the intervention to baseline and between immediately and one month after intervention.
The mean scores of the mentioned variables in the control group did not change significantly in three times. In comparison between study groups, except for the psychosocial domain, the mean scores of menopausal quality of life and its different domains differed significantly between the study groups one month after the intervention (Table 4).
Discussion
The results of the present study indicated the positive effect of holding six weekly self-awareness counseling sessions on improving the quality of life of menopausal women and their physical, vasomotor and sexual domains. In line with our results, Farokhi et al. (2015) reported that life skills training to the intervention group caused a significant improvement one month after the intervention between menopausal women of the two groups in the quality of menopausal life, their vasomotor and sexual domains except the physical and psychosocial domain (9).
In the present study, a clear improvement was also observed in the physical domain of quality of life of menopausal women that the difference between the two studies could be due to the difference in the content and duration of the sessions. In Farokhi study only one self-awareness session was taught to the intervention group. It seems that in the present study after training of six session’s self-awareness they were able to better adapt to the physical problems of menopause.
Forouhari et al. (2009) reported the positive effect of menopause education on the quality of life of menopausal women and all its domains of physical, sexual, vasomotor and psychosocial three months after the intervention in between two groups of women (10). The results of the mentioned study were consistent with the present study except for the psychosocial domain.
Despite the improvement of the psychosocial domain score in the present study, this improvement was not statistically significant. Perhaps it can be due to some items in the psychosocial domain, such as "dissatisfaction with personal life" that are influenced by external factors which in addition to gaining self-awareness skills, need more opportunities and practice to change attitudes and behaviors to overcome these factors. In addition, different content of intervention sessions and socio-cultural factors may justify the difference between the two studies. In the present study, quality of life during menopause improved in the intervention group but not in the control group.
Similarly, one study showed the positive effects of menopausal health education on negative attitudes about hot flashes as well as strengthen positive attitudes and increase menopausal quality of life six months after the intervention (20). Parsa et al. in their study reported that group counseling on menopause and self-care improved quality of life in menopausal women 3 months after counseling in the intervention group (21). In study of Karimy et al. also was reported improvement of quality of life of menopausal women after empowerment-based educational interventions (22).
Improved domain of psychosocial quality of life in the intervention group indicates that the self-awareness group counseling could reduce feelings such as depression, dissatisfaction with life, loneliness, impatience, poor memory, anxiety and anger, which could have negative effects on everyday life. However in the control group, there was no significant difference in improving the psychosocial domain of menopause after the intervention. Parsa et al. (2017) also reported a significant improvement in the psychosocial domain associated with menopause of intervention group women three months after group counseling (21).
In the present study, the sexual domain improved after the self-awareness intervention compared to baseline, a trend that continued until the end of the follow-up period. In the control group, no improvement in sexual domain was observed in no time. A study by Osinowo in Nigeria showed that education on menopause-related psychological factors could improve sexual activity and sexual satisfaction in menopausal women (23). We observed a significant improvement in the vasomotor domain of intervention group menopausal women immediately and one month after the intervention. Therefore, self-awareness counseling could reduce symptoms including discomfort, insomnia, anxiety and depression and increase self-esteem in menopausal women (4).
In another study, an empowerment-based education program on the awareness, attitude, self-esteem and self-efficacy of menopausal women significantly improved the vasomotor domain of menopausal women after two weeks (11). Despite decrease in mean score of the vasomotor domain (improvement) immediately after the intervention compared to baseline, we did not observe a significant statistically improvement. This confirms that self-awareness skills are acquired gradually over time.
In our study, the self-awareness group counseling also improved the physical domain of quality of life during menopause, which is in line with results of other studies in Iran (10, 21). Overall, the study findings indicate that the self-awareness group counseling positively affected the quality of life of menopausal women in Gorgan.
Conclusion
Based on the results, we recommend offering self-awareness counseling in health centers for improving the quality of life of menopausal women. Since the quality of life of menopausal women is influenced by various factors, it was impossible to control all human factors. It is suggested to study the effect of self-awareness group counseling on the quality of life of menopausal women at different periods of menopause and ethnicities groups.
Acknowledgements
We are grateful to the Research Deputy of Golestan University of Medical Sciences, Faculty of Nursing and Midwifery, and all participants for their cooperation.
Funding source
The manuscript has been derived from results of a master's thesis in midwifery counseling funded by the Reproductive Health and Midwifery Research Center of Golestan University of Medical Sciences.
Ethical statement
The study protocol was approved by the Ethics Committee of Golestan University of Medical Sciences (ethical code: IR.GOUMS.REC.1397.041) and was registered in IRCT (IRCT20180613040092N1).
Conflict of interest
The authors declare that there is no conflict of interest.
The results of the present study indicated the positive effect of holding six weekly self-awareness counseling sessions on improving the quality of life of menopausal women and their physical, vasomotor and sexual domains. In line with our results, Farokhi et al. (2015) reported that life skills training to the intervention group caused a significant improvement one month after the intervention between menopausal women of the two groups in the quality of menopausal life, their vasomotor and sexual domains except the physical and psychosocial domain (9).
In the present study, a clear improvement was also observed in the physical domain of quality of life of menopausal women that the difference between the two studies could be due to the difference in the content and duration of the sessions. In Farokhi study only one self-awareness session was taught to the intervention group. It seems that in the present study after training of six session’s self-awareness they were able to better adapt to the physical problems of menopause.
Forouhari et al. (2009) reported the positive effect of menopause education on the quality of life of menopausal women and all its domains of physical, sexual, vasomotor and psychosocial three months after the intervention in between two groups of women (10). The results of the mentioned study were consistent with the present study except for the psychosocial domain.
Despite the improvement of the psychosocial domain score in the present study, this improvement was not statistically significant. Perhaps it can be due to some items in the psychosocial domain, such as "dissatisfaction with personal life" that are influenced by external factors which in addition to gaining self-awareness skills, need more opportunities and practice to change attitudes and behaviors to overcome these factors. In addition, different content of intervention sessions and socio-cultural factors may justify the difference between the two studies. In the present study, quality of life during menopause improved in the intervention group but not in the control group.
Similarly, one study showed the positive effects of menopausal health education on negative attitudes about hot flashes as well as strengthen positive attitudes and increase menopausal quality of life six months after the intervention (20). Parsa et al. in their study reported that group counseling on menopause and self-care improved quality of life in menopausal women 3 months after counseling in the intervention group (21). In study of Karimy et al. also was reported improvement of quality of life of menopausal women after empowerment-based educational interventions (22).
Improved domain of psychosocial quality of life in the intervention group indicates that the self-awareness group counseling could reduce feelings such as depression, dissatisfaction with life, loneliness, impatience, poor memory, anxiety and anger, which could have negative effects on everyday life. However in the control group, there was no significant difference in improving the psychosocial domain of menopause after the intervention. Parsa et al. (2017) also reported a significant improvement in the psychosocial domain associated with menopause of intervention group women three months after group counseling (21).
In the present study, the sexual domain improved after the self-awareness intervention compared to baseline, a trend that continued until the end of the follow-up period. In the control group, no improvement in sexual domain was observed in no time. A study by Osinowo in Nigeria showed that education on menopause-related psychological factors could improve sexual activity and sexual satisfaction in menopausal women (23). We observed a significant improvement in the vasomotor domain of intervention group menopausal women immediately and one month after the intervention. Therefore, self-awareness counseling could reduce symptoms including discomfort, insomnia, anxiety and depression and increase self-esteem in menopausal women (4).
In another study, an empowerment-based education program on the awareness, attitude, self-esteem and self-efficacy of menopausal women significantly improved the vasomotor domain of menopausal women after two weeks (11). Despite decrease in mean score of the vasomotor domain (improvement) immediately after the intervention compared to baseline, we did not observe a significant statistically improvement. This confirms that self-awareness skills are acquired gradually over time.
In our study, the self-awareness group counseling also improved the physical domain of quality of life during menopause, which is in line with results of other studies in Iran (10, 21). Overall, the study findings indicate that the self-awareness group counseling positively affected the quality of life of menopausal women in Gorgan.
Conclusion
Based on the results, we recommend offering self-awareness counseling in health centers for improving the quality of life of menopausal women. Since the quality of life of menopausal women is influenced by various factors, it was impossible to control all human factors. It is suggested to study the effect of self-awareness group counseling on the quality of life of menopausal women at different periods of menopause and ethnicities groups.
Acknowledgements
We are grateful to the Research Deputy of Golestan University of Medical Sciences, Faculty of Nursing and Midwifery, and all participants for their cooperation.
Funding source
The manuscript has been derived from results of a master's thesis in midwifery counseling funded by the Reproductive Health and Midwifery Research Center of Golestan University of Medical Sciences.
Ethical statement
The study protocol was approved by the Ethics Committee of Golestan University of Medical Sciences (ethical code: IR.GOUMS.REC.1397.041) and was registered in IRCT (IRCT20180613040092N1).
Conflict of interest
The authors declare that there is no conflict of interest.
Author contributions
MSH collected and analyzed the data and wrote the manuscript. TZ supervised the study, critically revised the manuscript and provided comments about the manuscript. MT interpreted the data, revised the manuscript and provided comments about the manuscript. EKH supervised the study and participated in all part of study including designing the study, data analysis and manuscript writing. The author(s) read and approved the final manuscript.
Type of study: Original Article |
Subject:
Midwifery
References
1. Fallahzade H, Dehghani Tafti A, Dehghani Tafti M, Hoseini F, Hoseini H. Factors Affecting Quality of Life after Menopause in Women, . JSSU. 2011; 18 (6):552-558. [Persian] [View at paplisher] [Google Scholar]
2. Blumel JE, Castelo-Branco C, Binfa L, Gramegna G, Tacla X, Aracena B, et al. Quality of life after the menopause: a population study. Maturitas. 2000; 34(1):17-23. [View at paplisher] [DOI] [Google Scholar]
3. Im E-O, Im Lee B, Chee W, Dormire S, Brown A. A national multiethnic online forum study on menopausal symptom experience. journal Nursing research. 2010; 59(1):26-33. [View at paplisher] [DOI] [PMID] [Google Scholar]
4. Abdi N, Solhi M. Quality of life in postmenopausal women in Tehran. Iranian Journal of Health Education and Health Promotion. 2014; 2(2):87-96. [Persian] [View at paplisher] [Google Scholar]
5. Nazarpour S, Simbar M, Ramezani Tehrani F, Alavi Majd H. Quality of life and sexual function in postmenopausal women. Journal of women & aging. 2018; 30(4):299-309. [View at paplisher] [DOI] [PMID] [Google Scholar]
6. Webster AD, Finstad DA, Kurzer MS, Torkelson CJ. Quality of life among postmenopausal women enrolled in the Minnesota Green Tea Trial. Journal Maturitas. 2018; 108:1-6. [View at paplisher] [DOI] [PMID] [Google Scholar]
7. Yoshany N, Bahri N, Morovati Sharif Abad M, Mihanpour H, Delshad Noghabi A. Effects of Training the Menopausal Health on Knowledge and Performance of Husbands with Women during Transitional Period to Menopause. j.health. 2018; 9 (1):27-35.[Persian] [View at paplisher] [Google Scholar]
8. Khavandizadeh Aghdam S, Kazemzadeh R, Mahfouzi Y. Effectiveness of Education on Life Style in Menopausal Women. sjimu. 2018; 26 (1):43-51 [Persian] [View at paplisher] [DOI] [Google Scholar]
9. 9 Farokhi F, Narenji F, Salehi B, Mehrabi F, Rafiei M. Effect of skill life training in quality of life in menopausal women. Avicenna J Nurs Midwifery Care. 2015; 23 (4):54-64. [Persian] [View at paplisher] [Google Scholar]
10. Forouhari S, Safari Rad M, Moattari M, Mohit M, Ghaem H. The effect of education on quality of life in menopausal women referring to Shiraz Motahhari clinic in 2004. J Birjand Univ Med Sci. 2009; 16 (1):39-44. [Persian] [View at paplisher] [Google Scholar]
11. Moridi G, Seyedalshohadaee F, Hossainabasi N. The effect of health education on knowledge and quality of life among menopause women. Iran Journal of Nursing. 2006; 18(44):31-8. [Persian] [View at paplisher] [Google Scholar]
12. Thornton WJ, Dumke HA. Age differences in everyday problem-solving and decision-making effectiveness: A meta-analytic review. journal Psychology and aging. 2005; 20(1):85. [View at paplisher] [DOI] [PMID] [Google Scholar]
13. Jack K, Miller E. Exploring self-awareness in mental health practice. journal Mental Health Practice. 2008; 12(3):31-6. [View at paplisher] [DOI] [Google Scholar]
14. Hoseinkhanzadeh Abbasali, Malekimanesh Arezoo, Taher Mahboubeh, Mojarad Arezoo. The Effect of Self-Awareness Training on Reducing Aggressive Behavior, Addiction and Suicide of High School Girl Students. Journal New Thoughts on Education 2018:135 to 157. [Persian] [View at paplisher] [Google Scholar]
15. Ownsworth TL, McFarland K, Young RM. The investigation of factors underlying deficits in self-awareness and self-regulation. journl Brain Injury. 2002; 16(4):291-309. [View at paplisher] [DOI] [PMID] [Google Scholar]
16. Bögels SM, Rijsemus W, De Jong PJ. Self-focused attention and social anxiety: The effects of experimentally heightened self-awareness on fear, blushing, cognitions, and social skills. Journal Cognitive Therapy and Research. 2002; 26(4):461-72. [View at paplisher] [DOI] [Google Scholar]
17. Bauld R, Brown RF. Stress, psychological distress, psychosocial factors, menopause symptoms and physical health in women. Journal Maturitas. 2009; 62(2):160-5. [View at paplisher] [DOI] [PMID] [Google Scholar]
18. Moradpoor J. Effectiveness of training self-awareness and assertiveness skills on self-esteem and compatibility of mothers of mentally retarded children. Modern care journal. 2013. [Persian] [View at paplisher] [Google Scholar]
19. Fata l, Motaby F, Khany SM. Life skills training for student Tehran: Danzhh; 2007. 208 p.
20. Sis Çelik A, Pasinlioğlu T. Effects of imparting planned health education on hot flush beliefs and quality of life of climacteric women. journal Climacteric. 2017; 20(1):25-30. [View at paplisher] [DOI] [PMID] [Google Scholar]
21. Parsa P, Tabesh RA, Soltani F, Karami M. Effect of group counseling on quality of life among postmenopausal women in Hamadan, Iran. J Menopausal Med. 2017; 23(1):49-55. [View at paplisher] [DOI] [PMID] [Google Scholar]
22. Karimy m. Evaluation of the effect of educational intervention based on empowerment model of health promotion behaviors on menopautic women. daneshvar medicine. 2011; 19(3):73-80. [Persian] [View at paplisher] [Google Scholar]
23. Osinowo HO. Psychosocial factors associated with perceived psychological health, perception of menopause and sexual satisfaction in menopausal women and controls. West African journal of medicine. 2003; 22(3):225-31. [View at paplisher] [DOI] [PMID] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
