
Volume 18, Issue 1 (5-2021)
J Res Dev Nurs Midw 2021, 18(1): 49-52 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ziaei T, Gholipour S, Danesh A. The Effect of Group Counseling based on Communication Skills on the Quality of Life of Pregnant Women. J Res Dev Nurs Midw 2021; 18 (1) :49-52
URL: http://nmj.goums.ac.ir/article-1-1097-en.html
URL: http://nmj.goums.ac.ir/article-1-1097-en.html



1- Associate professor , Counseling and Reproductive Health Research Center, Department of Midwifery and counseling in midwifery, Golestan University of Medical Sciences, Gorgan, Iran
2- Counseling and Reproductive Health Research Center , Department of Midwifery, School of Gorgan Nursing & Midwifery, Golestan University of Medical Sciences, Gorgan, Iran ,somayeh_gholipoor@yahoo.com
3- Golestan Research Center of Psychiatry (GRCP), Golestan University of Medical Sciences, Gorgan, Iran
2- Counseling and Reproductive Health Research Center , Department of Midwifery, School of Gorgan Nursing & Midwifery, Golestan University of Medical Sciences, Gorgan, Iran ,
3- Golestan Research Center of Psychiatry (GRCP), Golestan University of Medical Sciences, Gorgan, Iran
Full-Text [PDF 694 kb]
(1868 Downloads)
| Abstract (HTML) (4394 Views)
Abstract
Full-Text: (1076 Views)
Abstract
Background: Women experience psychological problems during pregnancy affecting their quality of life. Since weakness in life skills, including communication skills (CS), is a factor of reducing the quality of life, we conducted a study to determine the effect of group counseling based on communication skills on the quality of life in pregnant women in Gorgan.
Methods: The parallel randomized field study trial carried out in 2016 on 72 pregnant women who referred to the health centers in Gorgan, Iran. The pregnant women at the gestational age of 14-18 weeks were recruited in convenience sampling method, and then randomly assigned in to the intervention and control groups using the block randomization method. The data collection tool included the quality of life questionnaire (SF-36) that was completed by both groups before the intervention. The samples of the intervention group received 6 sessions of group counseling based on communication skills for a one-hour session per week. A week after the sessions, the questionnaires were completed again by both groups. We analyzed the data in SPSS-16 using the independent t-test, Mann-Whitney test, Wilcoxon test, Paired t-test, and Chi-square test.
Results: The mean of women's age was 28.4±4.3 years in the intervention group, and was 26.8±4.5 years in the control group, and the mean age of their husbands were 33.14±5.3 and 31.22± 4.8 in the intervention and control groups, respectively. There was statistically significant difference between the intervention (60±15.2) and control (49±13.4) groups after the intervention in total quality of life (P=0.002). The results indicated that the mean scores of quality of life of women in the intervention group versus the control group after the intervention had statistically significant differences in all areas except for the "physical function" (65.3±17.4 vs. 61.5±20.1, P=0.4) and "role limitation due to physical problems" (50±36.8 vs. 45.1±27.3, P=0.56).
Conclusion: The health centers need to be taught about the communication skills in line with physical training during pregnancy by midwives and midwifery counselors.
Introduction
According to the World Health Organization (WHO), the quality of life is the individuals' perception of their positions in life in terms of culture, value system where they live, their goals, expectations, standards, and priorities; hence, it is a completely individual issue, cannot be seen by others, and is based on different aspects of life (1). Pregnant women are most sensitive groups in society because pregnancy is an important stage of a woman's life, and the quality of life significantly changes during this period (2). During this period, many biological, chemical, physiological, and anatomical changes occur in the body (3). Women experience psychological problems that can change their ability to perform normal life roles and reduce their quality of life during pregnancy compared to the non-pregnancy period (4, 5). Several studies have reported low quality of life in pregnancy (5). Jackson & Haas (2005) recommended the health care providers to consider the issue in their work (6). Makvandi et al. (2010) pointed out the low score of vitality as a quality of life dimension and the importance of planning and identifying factors that can improve this dimension of quality of life in future studies (7). Low quality of life affects family relationships, leads to the use of inefficient methods, increased stress, and consequently adversely affects their physical and mental health (8). King et al. (2005) pointed out the role of quality of life and efforts to improve it as an important factor in the personal and social life (9). Researchers have identified many factors that can affect the quality of life, including 1- Lack of effective life skills, 2- Styles of coping with stress, and 3- Inability to cope effectively with life problems (10). The ability to communicate is a complex issue that requires different knowledge and adequacy, including language adequacy (11). Given the humans' characteristics in the new age and the higher quality of life, the urgent need to acquire life skills for all human beings has been approved by authorities and planners in different countries. Life skills (self-awareness, empathy, communication skills, interpersonal relationships, decision making, problem solving, creative thinking, critical thinking, and coping with stress) are skills that can be taught to increase psycho-social abilities; they enable people to be able to effectively face with problems and conflict of life (12). Communication skills refer to the development of practical skills for individuals to learn how to adapt to the social environment and people who live in this environment and understand their feelings and opinions (13), and convey their feelings to others to achieve positive and pleasant results in themselves and others (14). Communication skills are also necessary for living and continuing the path and can be effective in dealing with others, and any shortcomings in this field can also cause problems, such as loneliness, social anxiety, depression, low self-esteem, and academic and occupational failure (15). Communication skills are about the way of action and behavior, and if they are practically taught, they will be able to improve the society by changing the individuals' behavior (16).
Rafiee (2009) reported the effectiveness of training on quality of life and psychological well-being in infertile women (17) and Fouladi et al. (2012) found the effect of communication skills training on improving women's quality of life (18). The communication skills play significant roles in increasing the marital adjustment and reducing the problems of intimate relations. There are a variety of interventional methods to achieve a high-quality life, one of which is the communication skills training (19). The individuals, who are influenced by life skills training, are more aware of their lives and abilities and are confident that they can go through the steps of progress and reach a higher level of development with effort (20).
Communication skills training creates a set of abilities in individuals and can pave the way for adaptation and positive behavior; hence, focus on improving communication skills and its progress through designing and holding the learning workshops can play an important role in the general health of learners (21).
The health centers of Iran provide the pregnancy care, but they emphasize the physical issues of pregnant women and pay less attention to psychological issues and quality of life of pregnant women. However, physical health requires mental health and high levels of quality of life. Since the pregnant women's mental health guarantees the family and social health, and these women are the educators of children and the next generation, it is very important to determine their quality of life and teach skills to improve their quality of life (22). The present study aimed to determine the effect of group counseling based on communication skills on the quality of life of pregnant women who visited the health centers of Gorgan.
Methods
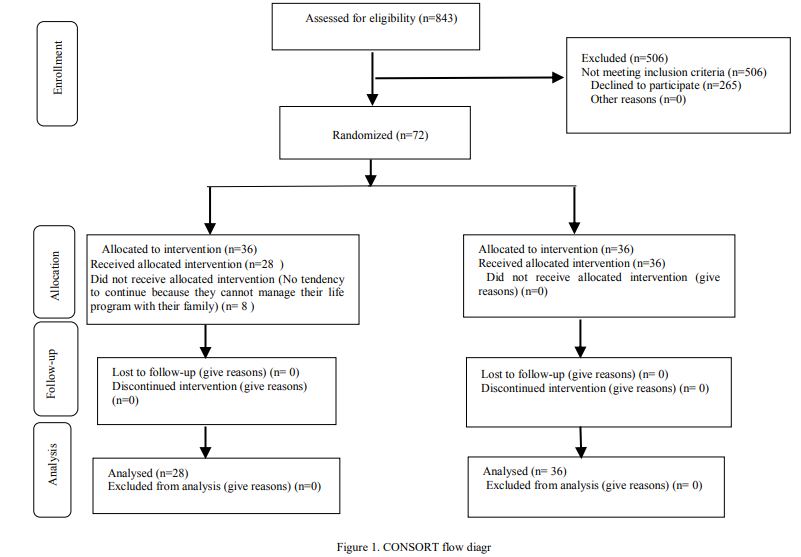
We conducted parallel randomized field trial with code of ethics (IR.GOUMS.REC.1394.345) on pregnant women who referred to the health care centers of Gorgan, Iran in 2016.The samples were selected from nine health centers of different regions of Gorgan using the convenience sampling method considering the inclusion criteria. Inclusion criteria were gestational age between 14-18 weeks, mothers' age between 18-35 years, no history of chronic diseases, no history of participation in training courses of communication skills, and no experience of grief and crisis in the past 3 months. They were explained about the purpose of the study and also assured about information confidentiality. The data collected using Quality Of Life Questionnaire (SF-36) (23). They filled out the questionnaires before being assigned to two groups. Overall, 72 out of 843 subjects were included in the study and allocated into two intervention in block randomization (n=36) and control (n=36) groups (Figure 1).
We held the communication skills-based group counseling 6 sessions per week, each lasted one hour, including the emotion classification, definition of effective communication, verbal and non-verbal elements of communication, barriers to communication, and active listening (Table 1) (24, 25). Both groups completed the questionnaires a week after intervention.
.png)
The sample size was calculated equal to 36 per group according to a study by Javadi and Sepahvand (2013) based on mean difference of scores of the SF-36 questionnaire between two groups (mean difference=12.8, SD=13.65), power of study 80%, the probability of type I error of 0.05%, and the following equation for dependent variables, and calculating 15% loss (26).

We utilized quality of life questionnaire (SF-36) with 36 items and eight dimensions; physical function (10 items), role Limitations due to physical problems (4 items), role Limitations due to emotional problems (3 items), energy/Vitality (4 items), mental health (5 items), social function (2 items), pain (2 items) and general health (5 items) and mental health (5 items).
Some items of the questionnaire were on a Likert scale and some had the "yes and no" type. To get the scores of 8 dimensions, the scores obtained from the items relating to each domain were added and then divided by the number of items. Therefore, the scores of each domain are ranging from 0 to 100). Higher scores indicate better health status. The validity and reliability of the Short Form 36 Health Survey Questionnaire (SF-36) were performed by Montazeri et al. We calculated the reliability test using the internal consistency method, and the Cronbach's alpha coefficient was from 0.77 to 0.90. The convergent validity test and factor analysis indicated that the correlation coefficients had a range of changes from 0.58 to 0.95 (27). The normality was first measured by Shapiro-Wilk test, in normal distribution data the independent t-test was used in between groups before and after the intervention, otherwise the Mann-Whitney test was used. Paired t-test or Wilcoxon test were used to compare before-and-after quality of life. Furthermore, the chi-square was used for husbands' jobs and education levels.
Eight out of 72 participants (34 in the intervention group and 34 in the control group) withdrew from the study due to their unwillingness to continue participating in counseling sessions, leading to a total of 64 individuals (28 in the intervention group, and 36 in the control group )( Figure 1).
Results
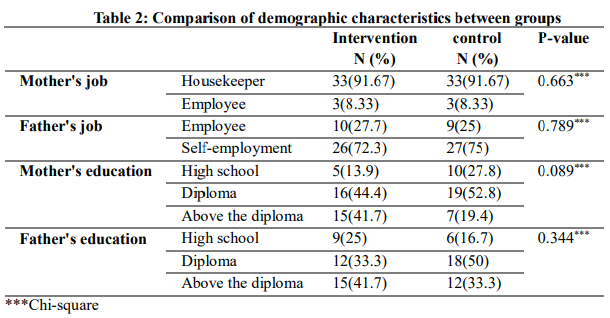
The mean±standard deviation of women's age was 28.4±4.3 years in the intervention group, and was 26.8±4.5 years in the control group, and the mean age of their husbands were 33.14±5.3 and 31.22±4.8 in the intervention and control groups, respectively. There was no statistically significant difference between the intervention and control groups in terms of the age of pregnant women and their husbands, number of children, job, pregnant women's education levels, and their husbands' jobs and education levels.
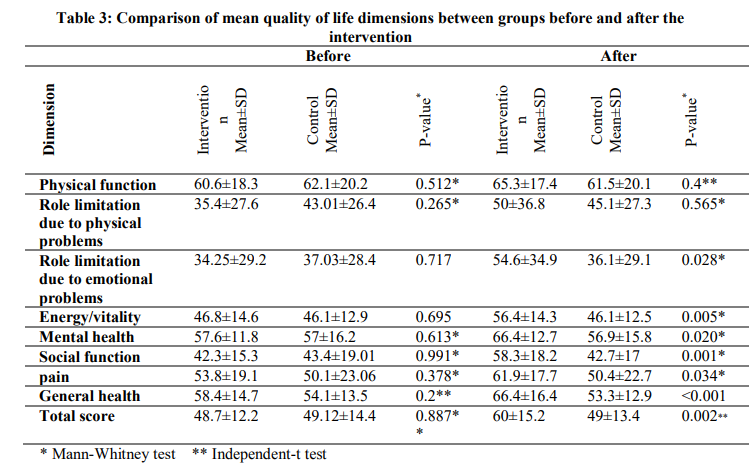
We compared the quality of life dimensions in the intervention and control groups before the intervention. The results indicated no statistically significant differences between the two groups before the intervention.
After the intervention, there were statistically significant differences between mean scores of quality of life of women in the intervention group and the control group in all domain except for the "physical function" (65.3±17.4 vs. 61.5±20.1) and "role limitations due to "Physical problems" (36±50.8. vs. 27.3±45.1). The total score of quality of life was significantly different between intervention (60.0± 15.2) and control (49.0±13.4) groups after the intervention (P= 0.002) (Table 2).
We evaluated the changes in quality of life scores between the two groups before and a week after the intervention to examine the effects of counseling sessions on the participants' quality of life, and the results indicated that the intervention in all dimensions and the overall quality of life except for the pain improved the quality of life in the intervention group (7.9±16.4) compared to the control group (0.27±9.6) (Table 4).

Discussion
Results of the present study indicated that there is no significant difference between the total mean scores of quality of life of pregnant women in the intervention and control groups before the intervention; however, there was a statistically significant difference in the intervention group compared to the control group after the intervention, and the quality of life score in the intervention group increased compared to the control group.
Results of the present study indicated that the two dimensions, "physical function" and "role limitation relating to physical health" as dimensions of quality of life, had no statistically significant differences in the two groups of intervention and control after the intervention. Sadeghi et al. (2012) conducted a study, titled "The effect of life skills training on dimensions of quality of life of adolescent orphans under the protection of Imam Khomeini Relief Foundation of Isfahan", and found that life skills training increased all aspects of quality of life except for the physical health (28), and the result was consistent with the present study.
The present study indicated that the "role limitation relating to the emotional health" as a dimension of quality of life was positively affected by communication skills counseling. Khodabakhsh et al. (2010) studied the effects of life skills training on the individuals' mental health and concluded that training increased their emotional health levels, and the result was consistent with the present study (29).
In the present study, the results indicated that communication skills training was effective in creating "energy" in pregnant women probably since the happiness produced energy and enthusiasm, and could protect people against stress and ensure their mental health. Since communication skills training increased happiness, the positive role of training could be understood in increasing energy levels in the individuals. Sepehrnia et al. (2010) also found that life skills training significantly increased the quality of life of diabetic patients, especially in the field of "energy" (30). Since communication skills training increased happiness, which happiness produced energy and enthusiasm and could protect people against stress and ensure their mental health, the positive role of training could be understood in in increasing energy levels in the individuals.
The results also indicated that communication skills training was effective in "social function" of pregnant women probably because the individuals gradually learn how to communicate properly with people in this small community by attending group counseling sessions and interacting with other people in the group, and the experience helped them understand how to adapt to a bigger social environment and those who were living in that environment, and how to increase their social functions. Rezapour Mirsaleh et al. (2016), who examined the effectiveness of intervention based on life skills training on the quality of life of female heads of households under the protection of the welfare organization, reported significant effect in the "social function" domain (12). Results of the present study also indicated that communication skills training was effective in reducing the "physical pain" on the pregnant women. Javadi et al. (2012) also found that life skills training significantly improved the nurses' physical pain (26), and their results were consistent with the present study.
The present study also indicated that communication skills training was effective in "general health" of pregnant women probably because the higher life skills created accountability to health care, made good decisions about health, and generally led to healthy lifestyles among learners so that they would be prepared to deal with life changes and needs in the future. Fouladi et al. (2013) found results consistent with the present study, indicating the effectiveness of communication skills training in improving general health as a domain of quality of life in married women (18).
Conclusion
Due to the positive effect of group counseling based on communication skills on the quality of life of pregnant women in Gorgan, we suggest providing this counseling along with other services by midwives in midwifery centers and offices to improve the quality of life of pregnant women.
A limitation of the present research was the completion of questionnaires as a self-report that increased the possibility of concealment and implicit reflection of the reality. The present study also indicated the short-term effects of the intervention and did not include its long-term effects; hence, subsequent studies should provide a long-term follow-up.
Acknowledgements:
We are grateful to the research and technology deputy of Golestan University of Medical Sciences for their great cooperation and funding for conducting the research, as well as the staff of health centers in Gorgan and the esteemed women who participated in the study.
Funding source:
This research did not receive any grant from funding agencies.
Ethical statement:
This study was approved by the ethics committee of the Golestan University of Medical Sciences.
Conflict of interest:
The authors declared no conflict of interest.
Author contributions
Conceptualization: Tayebe Ziaei, Somayeh Gholipour. Methodology,
analysis, research review and editing: Tayebe Ziaei, Somayeh Gholipour,Ahmad Danesh. Writing: Tayebe Ziaei, Somayeh Gholipour Supervision: Tayebe Ziaei
Type of study: Original Article |
Subject:
Midwifery
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
