
Volume 18, Issue 1 (5-2021)
J Res Dev Nurs Midw 2021, 18(1): 21-25 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Haidari Z, Modanloo M, kazemi S B, Farzadmehr M. Comparison of the Effects of Face-to-Face and Group Education on Awareness and Anxiety of Family Members of Candidates for Coronary Angiography. J Res Dev Nurs Midw 2021; 18 (1) :21-25
URL: http://nmj.goums.ac.ir/article-1-1186-en.html
URL: http://nmj.goums.ac.ir/article-1-1186-en.html



1- Intensive Care Nursing, Golestan University of Medical Sciences, Gorgan, Iran
2- Department of Psychiatry and Community Health Nursing, School of Nursing and Midwifery Golestan University of Medical Sciences, Gorgan, Iran
3- Health care Management.G olestan Univercity of Medical Sceinces. Gorgan, Iran
4- psyachtric Nursing, Shaheed Sayyad Shirazi academic and research center, Gorgan, Iran , farzadmehr87@yahoo.com
2- Department of Psychiatry and Community Health Nursing, School of Nursing and Midwifery Golestan University of Medical Sciences, Gorgan, Iran
3- Health care Management.G olestan Univercity of Medical Sceinces. Gorgan, Iran
4- psyachtric Nursing, Shaheed Sayyad Shirazi academic and research center, Gorgan, Iran , farzadmehr87@yahoo.com
Keywords: Face-to-Face education [MeSH], Group education , Anxiety , Awareness [MeSH], Coronary angiography [MeSH]
Full-Text [PDF 660 kb]
(834 Downloads)
| Abstract (HTML) (1985 Views)
Abstracta
Full-Text: (696 Views)
Abstracta
Background: Coronary angiography causes anxiety in patients and family that is a major cause of anxiety and lack of awareness. Choosing the right educational method is effective in increasing family awareness and support of patients. The present study aimed to compare the effects of Face-to-Face and group education on awareness and anxiety of family members of candidates of coronary angiography.
Methods: This randomized clinical trial study was conducted on 90 family members of candidates of coronary angiography at Amiralmomenin Hospital of Kordkuy as a referral center in Northeast of Iran in 2017. Eligible family member of patients was recruited through convenience sampling method and then allocated three; face-to-face education (A), group education (B), and control groups randomly. Family members in both intervention groups received same educational content about the method of performing coronary angiography, and the necessary care. The control group only received routine information. Data were collected using the Spielberger State-Trait Anxiety Inventory (STAI) and awareness questionnaire. SPSS Statistics for Windows, version x.0 (SPSS Inc., Chicago, Ill., USA). Software using descriptive statistics, paired t-test, Chi-square, Wilcoxon, and Kruskal-Wallis tests. The significance level was considered less than 0.5.
Results: The score of anxiety and awareness in patients’ family members were not significantly different in the three groups before the intervention. After intervention, the mean scores of anxiety were 42.12±4.71 and 42.37±5.53 in the participants of group A and B respectively, and it was significantly different from the pre-intervention score (P<0.001). The mean awareness score was significantly higher in group B than in the other two groups (P<0.001).
Conclusion: According to the results, group education was more effective than face-to-face education in increasing awareness and reducing anxiety in families. We suggest developing programs in this regard.
Introduction
Coronary artery diseases are major health problems in today's society (1). In Iran, the highest mortality rate is related to cardiovascular diseases so that they account for about 40 percent of all deaths in society (2). Coronary angiography is a common invasive and diagnostic test that is considered the best and most accurate method and standard in the diagnosis of coronary artery diseases (3). Invasive diagnostic procedures such as angiography have been increasing due to the increase in coronary artery diseases in recent years. Research has indicated that the diagnosis and treatment of coronary artery diseases and the need for angiography have always led to fear and anxiety of patients and their families (4) and it can have negative consequences for the care of patients by the family. Furthermore, family members' anxiety can cause anxiety to transfer to the patient. Research indicates that the lack of information about angiography procedures and care before and after it, and fear of problems during the procedure are the most common causes of anxiety in families (5). Therefore, it is important to plan and implement a support program to reduce anxiety before performing an angiography procedure (6). Effective education has not been provided in medical centers of Iran according to the research and due to the time-consuming nature of the education process, and lack of sufficient human resources (7). Furthermore, candidates for angiography and angioplasty have a shorter hospital stay than patients with coronary artery bypass graft surgery that is also challenging because the possibility of psychological interventions is lower and less education is provided for patients and their families in this short period (2) Löfvenmark acknowledged that if a patient was unable to participate in training programs, it was important to involve the patient's attendants in education programs and care decisions. It can improve the quality of life and increase patients' awareness and consequently improve their adherence to the treatment regimen and reduce fatigue and confusion in caregivers. Therefore, given that the family plays an important role in improving the patient's health and mood, nurses need to pay attention to the patients in addition to family members and plan to meet their information needs. Therefore, the families' awareness and support can increase and their care-support capacity can be used in patient care by proper planning and selection of appropriate educational methods and correct training for them (8). Meanwhile, even though all approaches to education such as Face-to-Face and group education can affect the rates of learning and adaptation to stressful conditions of diseases, it is necessary to consider the purposes of education, personnel, and financial resources before deciding on the method of education (9). Face to face training and group discussions are the most common education approaches in health education programs. According to health education bases, face to face method has a greater effect on patients than other methods (10). This method also has a valuable place in people with low levels of understanding and education (11), but it is impossible to use face to face education in most situations due to the lower available resources, equipment, and workforce so that other education methods like group discussion should be used (10). Accordingly, since the researchers were working in Amiralmomenin Hospital of Kordkuy and there were a large number of patients' families with worries and anxieties behind the door of the angiography, they asked questions and sought to solve their ambiguities by visiting medical staff. Considering the busy nursing staff and the lack of sufficient opportunities for Face-to-Face education of each patient and family, the present study aimed to compare group and Face-to-Face education on the awareness and anxiety of family members of candidates for coronary angiography (8).
Methods
The randomized clinical trial was conducted on 90 family members of patients who candidates for coronary angiography at Amiralmomenin Hospital of Kordkuy affiliated to the Golestan University of Medical Sciences in northeastern Iran in 2017. The sample size was calculated to be 90 based on the formula at a 95% confidence level and 80% power (10, 32). Participants were recruited using the convenience sampling method considering the inclusion criteria. Then, they allocated into three; face-to-face education (A), group education (B), and control groups, randomly. To prevent information exchange of participants, sampling of different groups was done in intermittent periods. To this end, sampling was performed in group B and then in the control group respectively after sampling in the group A. Sampling lasted from October to the end of December 2017. Inclusion criteria were age >18 years, the patient's attendance during the angiography, the ability to read and write Persian, not be a healthcare providers, schedule for elective angiography, and not having psychiatric or anxiety disorders. Before sampling, informed consent was obtained from participants while giving explanations about the research and its goals. The intervention was done for patients' attendants in both intervention groups. The educational content was the same in both intervention groups included training on the purpose of angiography, its method, procedure duration, and its post and pre-care. It should be noted that the content validity of the curricula was evaluated by experts. The intervention method was done using Face-to-Face method in groups A in a 25-30-minute training session and 15 minutes of the necessary practical training by the researcher for participants. They were also given 10-15 minutes to exchange information, express their ideas to clarify the information, and ask and answer the questions. For participants in the A group, training was provided at the patient's bedside during 15 minutes. Ten minutes were considered for questions and answers. The control group received routine training. For participants in the B group training was provided in the small groups (6-8 participants) with the same content. To comply with the ethical principles after the completion of the questionnaires by the control group, the training was provided for the participants in the control group after data gathering. The data collected using demographic questionnaire, Spielberger State-Trait Anxiety Inventory (STAI), and the awareness questionnaire. The anxiety and awareness levels were once measured in A, B, and control groups during the hospitalization of the angiography for candidates and then two hours before the angiography by a researcher who had no information about the participants’ allocation in groups. Demographic information included age, sex, education, occupation, and family relativity with the patients. The STAI was designed by Spielberger in 1983. The questionnaire composed of 20 items, each rated on a 4-point Likert scale (1=never to 4=always). Ten items with direct expressions had scores of 1 to 4 and 10 items with inverse expressions received scores of 1 to 4 respectively. Thus, total scores range from 20 to 80. Higher scores indicate a higher anxiety, which the scores of 20-39 were put in the mild anxiety group, 40-59 in the moderate anxiety group, and 60-80 in the severe anxiety group (12). The validity and reliability were approved in different studies (13, 14). The awareness questionnaire was designed and used by Mohammadi et al. (2012) and its content validity and reliability of 0.81 were obtained (10). The questionnaire consisted of 17 four-choice questions. The lowest and highest scores obtained from the awareness questionnaire were 0 and 17, respectively. To determine the awareness score based on 100, the total score of the questionnaire was multiplied by 100 and divided by 17, and thus we divided the participants' awareness in the study into three categories, namely the poor awareness (score of 0-35), moderate awareness (score of 35-70), and high awareness (score of 70-100). We analyzed the data using the paired t-test, Chi-square test, Wilcoxon, and Kruskal-Wallis tests in the SPSS Statistics for Windows, version x.0 (SPSS Inc., Chicago, Ill., USA).for at a significance level of 0.05.
Results
In the present study, the mean age of participants was 37.4±9.69 in the group a, 39.1±10.03 in the group B, and 36.7±9.8 in the control group. The majority of participants (55%) had a high school diploma (75.12%), were housewives (50.16%), and 62.92% had child-to-patient relativity. Comparisons indicated that all three groups, A, B and control groups were similar in terms of demographic characteristics such as age, sex, education, occupation, and relativity with patients and there was no statistically significant difference between them (Table 1).

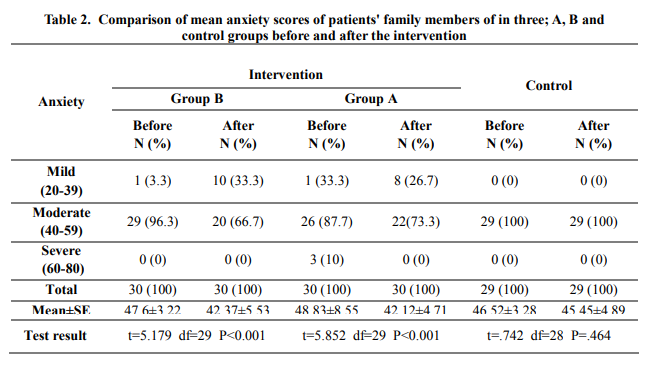
Participant (3.4%) in the control group left the study due to unwillingness to continue participating in the study and was excluded from the study. Before intervention, the anxiety scores were 55.63±3.22, 28.83±8.47, and 46.52±3.48 in three groups, A and B, and control groups respectively, and after intervention the anxiety scores were 42.12±4.713, 42.37±5.53, and 45.96±3.29 in the A, B, and control groups respectively In before intervention, the results indicated that there was no statistically significant difference in the family members' anxiety scores in the A and B, and control groups (P=0.34) (Table 2).
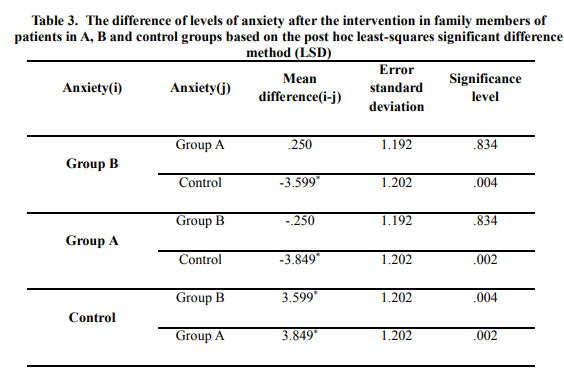
The difference between the mean anxiety of the participants in A, B and control was statistically significant after intervention (P=0.003), but the differences in anxiety in the A and B group were not significant (Table 3).
The results indicated that the mean awareness of the participants in group A, B, and control groups were the same in the before intervention and there was no statistically significant difference (P= 0.430). The comparison of the awareness levels of after intervention in the A, B, and control groups indicated a statistically significant difference (P=0.027) (Table 4). Considering the mean of the three groups after intervention, level of awareness score was higher in the B group (52.83) than the A (46.78) and control (35.05) groups (P=0.027).

Discussion
In the present study, we compared group and Face-to-Face education methods on the awareness and anxiety of family members of candidates for coronary angiography. The research results indicated that the group and Face-to-Face education intervention groups had higher awareness and lower anxiety than the control at the post-test stage. Comparing the post-test anxiety and awareness scores of the two intervention groups indicated that group education was more effective in increasing awareness than Face-to-Face education. Even though anxiety was lower in the intervention groups than the control group, the difference between the group and Face-to-Face education groups was not significant. Hospitalization and diagnostic and therapeutic interventions caused high levels of anxiety due to the complications and unknown environment for patients and family members (15- 17). The present study indicated that the majority of participants had moderate anxiety. The finding was consistent with other studies (16, 18- 20). The results of a study indicated that mean anxiety scores in the intervention group an hour before angiography and during the discharge day were less than the control group, and the result was consistent with results of the present study but the present study examined the anxiety in family members of angiography patients during hospitalization and two hours before angiography. (21) Furthermore, Saki et al. studies the reduction of anxiety through face-to-face and electronic education and found that the mean anxiety of patients was not statistically significant in the two groups even though the reduction of anxiety in the intervention groups was significant in comparison with the control group. Therefore, neither of these two education methods was superior to each other (22). Few studies have found that increasing the individuals' awareness of angiography may increase their anxiety. Astyle et al. studied angiographic anxiety reduction in Australia using three different methods, audio/visual, written, and oral (23). Researchers believe that different intervention methods should be studied and examined to detect and reduce the psychological problems of family members of patients admitted to the intensive care unit of angiography. Furthermore, the use of appropriate education methods is significantly important in health-oriented educational interventions (16, 23, 24, and 25). The use of an appropriate method helps to transfer content better leading to the higher efficiency of an intervention program (19). In Azarfarin's study, the use of information cards was useful in reducing the family members' anxiety in the waiting room for angiography and surgery (16). Obviously, due to the lack of any reference to answer the questions by patients' family members, they ask different groups of individuals in the hospital their medical questions; hence, they will be confused due to the lack of information or wrong information and different responses. To this end, family members cannot be sure of the provision of high-quality and acceptable medical and nursing services, and this can increase their levels of anxiety (26). Therefore, education is a more effective way to improve individuals' knowledge and awareness (3). Findings of a study by Mohammadi et al. indicated that group education was more effective on the anxiety of hospitalized patients for coronary angiography than Face-to-Face education. Their result was inconsistent with the present study; however, the present study examined the angiography patients' families (10). Bahrami's studies indicated that planned education significantly decreased the levels of stress and anxiety in family members of patients admitted to the intensive care unit (27). In a study by Riyazi et al., the results indicated that the education for pregnant mothers in the health system was mainly face to face, and sometimes in educational booklets and pamphlets, while group education not only took less time but also could convey a large amount of information to people due to having a regular schedule (28). In a study by Borimnejad et al., the group education had a greater effect than the individual learning on the follow-up of treatment by Warfarin users after the heart valve replacement (30). Results of studies on other fields have sometimes yielded conflicting results; for instance, a study by Ghavam-Nasiri on the emotional aspect of self-care in patients with diabetes in which there was a significant difference between the Face-to-Face and group education (p=0.394) (29). Education has been considered as the main task for nurses (31). According to the positions of Face-to-Face and group education, they are two main methods of organized education in health system employees (9, 29). The present results also indicated that each of the two educational methods decreased the family members' anxiety; hence, group education was more effective in increasing the family awareness than Face-to-Face education probably due to the higher motivation, the individuals' interaction with each other, using each other's experiences, providing an opportunity for sharing ideas and receiving support from the group in dealing with problems leading to higher awareness. Given that people in different cultures participate in the study, they may not express their feelings in critical and stressful situations and some cultural barriers may prevent them from expressing their true feelings; hence, we suggest that future studies with the same topics should pay attention to cultural factors affecting the research results.
Conclusion
The present study indicated that education could be effective in reducing anxiety and increasing awareness in family members of angiography patients. Education for the patients' attendants could increase their awareness, tolerance of the patients' families about the coronary angiography and its problems that could increase the patients' satisfaction and comfort, decrease complications and the length of stay in the hospital. Therefore, we suggest education for family members as a suitable strategy along with all treatment and support measures to improve the quality of life of patients and families.
Acknowledgements:
The authors gratefully acknowledge the participants for their time and effort to complete this study. Moreover, we are grateful to the administrators of the Amiralmomenin Hospital for their support. We would like to thank the Research Deputy of Golestan University of Medical Sciences., which financially supported this study
Funding source:
This study was approved and funded by Golestan University of Medical Sciences, Gorgan, Iran (Grant number: 960628155) and was approved Golestan University of Medical Sciences (code:IR.GOUMS.REC1396.159)
Ethical statement:
This study was approved by a committee for ethical research at Golestan University of Medical Science (code: IR.GOUMS.REC.1396.159) ) dated 19/09/2017 from the ethics committee of the university research council and a code IRCT 20190304042909 N1 registered on the Iranian Registry of Clinical Trials website All participants were agreed to participate in the study and signed a written informed consent before fulfilling the questionnaire .They were assured about confidentiality of private information and their voluntary for participation.
Conflict of interest:
None declared
Author contributions:
Z.H and M.F and S.K designed the project. M.F and Z.H collected and analyzed the data and wrote the manuscript Z.H and M.F and S.K and M.M participated in data analysis, supervised the study and critical revisions for important intellectual content. All the authors approved the content of the manuscript.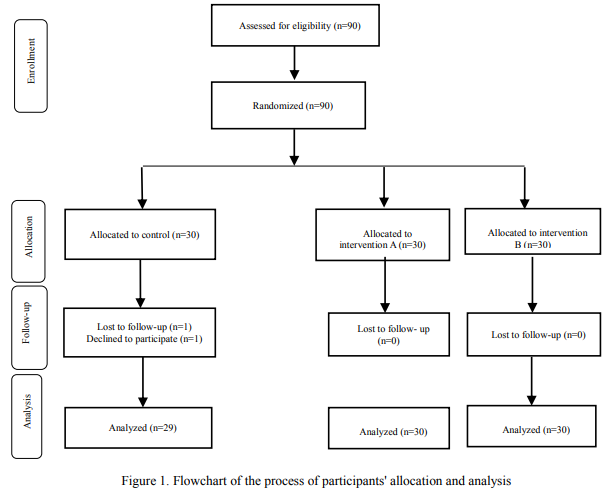
|
|
Type of Study: Original Article |
Subject:
Nursing
References
1. Hanifi, N. Bahraminezhad, N, MirzaeeT ,AhmadiF, Taran L. The effect of orientation program on stress, anxiety and depression of patients undergoing coronary angiography. 2012. 7 (25):1-8. [Persian] [View at paplisher] [Google Scholar]
2. Ebadi A, Moradian ST, Feyzi F, Asiabi M. Comparison of hospital anxiety and depression among patients with coronary artery disease based on proposed treatment. Iranian journal of critical care nursing. 2011. 4(2): 97-102. [Persian] [View at paplisher] [Google Scholar]
3. Brunner, L.S., Brunner & Suddarth's textbook of medical-surgical nursing. Vol. 1. 2010: Lippincott Williams & Wilkins.
4. Zafari S, Ghadrdoost B, Hanifi Z, Khaleghparast-Athari S. The effect of face-to-face education on knowledge, attitude, and believes of acute coronary syndrome patients about heart disease: an experimental study. Cardiovascular Nursing Journal. 2012; 1(1):36-41. [View at paplisher] [Google Scholar]
5. Sayin Y, Havva T, Hatice T-A, Yilmaz M. Anxiety of Relatives of Patients Undergoing Coronary Angiography, Stent, or Balloon Procedures. Hemşirelikte Araştırma Geliştirme Dergisi. 2014; 16(3):1-15. [View at paplisher] [Google Scholar]
6. Hajbaghery MA, Moradi T, Mohseni R. Effects of a multimodal preparation package on vital signs of patients waiting for coronary angiography. Nursing and midwifery studies. 2014; 3(1). [View at paplisher] [DOI] [Google Scholar]
7. Farsi Z, Sajadi SA, Eslami R. Effects of peer education and orientation tour on anxiety in patient candidates for coronary angiography. Nurs Midwifery Stud. 2016; 5(3): e31624. [View at paplisher] [DOI] [Google Scholar]
8. Löfvenmark C, Karlsson MR, Edner M, Billing E, Mattiasson A-C. A group-based multi-professional education programme for family members of patients with chronic heart failure: effects on knowledge and patients' health care utilization. Patient Education and Counseling. 2011; 85(2):e162-e8. [View at paplisher] [DOI] [Google Scholar]
9. Bolourchifard F, Neishabory M, AbedSaeedi Z. The effects of group and individual education on the level of the knowledge, attitude and practice of self care in patients with diabetic foot ulcer. Iran journal of nursing. 2009; 22(59):33-41. [Persian] [View at paplisher] [Google Scholar]
10. Mohammadi N, Tizhoosh M, Seyedoshohadaei M, Haghani H. Face-to-Face Education vs. Group education on knowledge and anxiety of patients undergoing coronary angiography. Journal of hayat. 2012; 18(3):44-53. [View at paplisher] [Google Scholar]
11. Zendehtalab H. Comparing the effect of face to face and group discussion teaching methods on quality of life improvement among patients suffering from multiple sclerosis. 2013; 13(9):711-720. [View at paplisher] [Google Scholar]
12. Mahmoudirad Gh. et al. Effect of foot reflexology on anxiety of patients undergoing coronary angiography. Iran J Crit Care Nurs. 2014; 6(4):235-242. [View at paplisher] [Google Scholar]
13. Jamalinik M, Maskani K, Koushan M, Rakhshani MH. The effect of group emotional expression on patient's anxiety about coronary angiography.Journal of SabzevarUniversity of Medical Sciences 2015; 22(4). [View at paplisher] [Google Scholar]
14. Dehghan-nayeri N, Adib-Hajbaghery M. Effects of progressive relaxation on anxiety and quality of life in female students: a non-randomized controlled trial. Complementary Therapies in Medicine. 2011; 19(4):194-200. [View at paplisher] [DOI] [Google Scholar]
15. Guo P, East L, Arthur A. A preoperative education intervention to reduce anxiety and improve recovery among Chinese cardiac patients: a randomized controlled trial. International journal of nursing studies. 2012; 49(2):129-37. [View at paplisher] [DOI] [Google Scholar]
16. Azarfarin R, Totonchi Z, Babaei M, Alizadehasl A, Ghadrdoost B, Najafikhah M, Ehsani A. Effectiveness of an "Information Card" in Reducing Family Members' Anxiety in the Waiting Room During Heart Surgery and Angiographic Procedures. Iranian Heart Journal. 2018 Jan 1; 19(2):65-70. [View at paplisher] [Google Scholar]
17. Shoushi F, Jannati Y, Mousavinasab NA, Shafipour V. The impact of family centered care on depression, anxiety and stress of family caregivers of patients undergoing open heart surgery. Iranian Journal of Rehabilitation Research. 2017; 3(2):53-60. [View at paplisher] [Google Scholar]
18. Muldoon M, Cheng D, Vish N, Dejong S, Adams J. Implementation of an informational card to reduce family members' anxiety. AORN journal. 2011 Sep 1; 94(3):246-53. [View at paplisher] [DOI] [Google Scholar]
19. Fallahi Khoshknab M, Farzadmehr M, Hosseini M A, Khankeh H R, NoorAbadi Z. Nursing Consultation on Anxiety of Patient's Family in Cardiac Surgery Intensive Care Unit. J Res Dev Nurs Midw. 2016; 12 (S3):1-8. [View at paplisher] [Google Scholar]
20. Imanipour M, Heidari Z, Seyedfatemi N, Haghani H. Effectiveness of informational support on anxiety among family carers of patients undergone open heart surgery. Journal of hayat. 2012; 18(3):33-43. [Persian] [View at paplisher] [Google Scholar]
21. Sh V, Keshavarz S, Nikbakhtnasrabadi A, Shamsizadeh M, Kazemnejad A. The effect of orientation tour with angiography procedure on anxiety and satisfaction of patients undergoing coronary angiography. Iranian Journal of Psychiatric Nursing. 2013; 1(2):1-10. [Persian] [View at paplisher] [Google Scholar]
22. Saki A, Hooshmand Bahabadi A, Asadi Noghabi AA, Mehran A. Comparison of Face-to-Face and Electronic Education Methods on Anxiety in Patients with Acute Myocardial Infarction. Hayat. 2014; 20(1). [Persian] [View at paplisher] [Google Scholar]
23. Astley CM, Chew DP, Aylward PE, Molloy DA, De Pasquale CG. A randomised study of three different informational AIDS prior to coronary angiography, measuring patient recall, satisfaction and anxiety. Heart, Lung and Circulation. 2008; 17(1):25-32. [View at paplisher] [DOI] [Google Scholar]
24. Jamshidi N, Abbaszadeh A, Kalyani MN, Sharif F. Effectiveness of video information on coronary angiography patients' outcomes. Collegian. 2013; 20(3):153-9. [View at paplisher] [DOI] [Google Scholar]
25. Hamester L, Souza ENd, Cielo C, Moraes MA, Pellanda LC. Effectiveness of a nursing intervention in decreasing the anxiety levels of family members of patients undergoing cardiac surgery: a randomized clinical trial. Revista latino-americana de enfermagem. 2016; 24. [View at paplisher] [DOI] [Google Scholar]
26. Trecartin K, Carroll DL. Nursing interventions for family members waiting during cardiac procedures. Clinical nursing research. 2011; 20(3):263-75. [View at paplisher] [DOI] [Google Scholar]
27. Bahrami F, Islami M, Moshtagh Eshgh Z, Fesharaki M. Effects of programmed education on stress of family careers with a relative in an intensive care unit of Isfahan University of Medical Sciences hospitals during 2009. Community Health Journal. 2017; 3(4):18-24. [View at paplisher] [Google Scholar]
28. Bahrami F, Islami M, Moshtagh Eshgh Z, Fesharaki M. Effects of programmed education on stress of family careers with a relative in an intensive care unit of Isfahan University of Medical Sciences hospitals during 2009. Community Health Journal. 2017; 3(4):18-24. [View at paplisher] [Google Scholar]
29. Ghavam-Nasiri M-R, Heshmati Nabavi F, Anvari K, Habashi Zadeh A, Moradi M, Neghabi G, et al. The effect of individual and group self-care education on quality of life in patients receiving chemotherapy: A randomized clinical trial. Iranian Journal of Medical Education. 2012;11(8):874-84.[persian] [View at paplisher] [Google Scholar]
30. Borimnejad L, Asemi S, Samiei N, Haghani H. Comparison of group and individual training on the patients' compliance and incidence of warfarin side effects after cardiac valve replacement. Iranian Journal of Medical Education. 2012; 12(1):10-8. [Persian] [View at paplisher] [Google Scholar]
31. Heidari M, Delaram M, Aliakbari F. Effect of nurse-led group educational sessions on the quality of lifeamong patients with implanted pacemakers. Journal of Urmia Nursing And Midwifery Faculty. 2012; 10(3). [View at paplisher] [Google Scholar]
32. Ivarsson B, Larsson S, Lührs C, Sjöberg T. Serious complications in connection with cardiac surgery-Next of kin's views on information and support. Intensive and Critical Care Nursing. 2011; 27(6):331-7. [View at paplisher] [DOI] [Google Scholar]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
